
View sample World Health Organization research paper. Browse research paper examples for more inspiration. If you need a health research paper written according to all the academic standards, you can always turn to our experienced writers for help. This is how your paper can get an A! Feel free to contact our writing service for professional assistance. We offer high-quality assignments for reasonable rates.
Founding And Mission
The World Health Organization (WHO) was established on 7 April 1948 as a specialized agency of the United Nations (UN), and the global authority on health issues. It came into existence when 26 of its 61 founding states signed its constitution. This day is marked as World Health Day.
Academic Writing, Editing, Proofreading, And Problem Solving Services
Get 10% OFF with 24START discount code
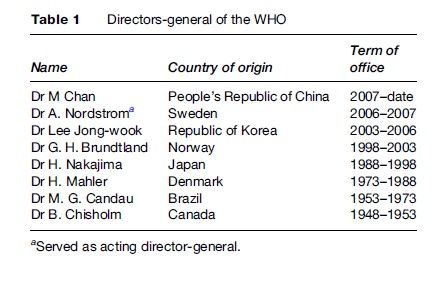
In the post-World War II era the global implications of poor health were recognized. As a result, Brazil and China put forward a joint declaration at the 1945 United Nations Conference on International Cooperation. This declaration called for a conference to look into the establishment of a global health agency; approval was unanimous. In 1946 a series of conferences were convened, leading to the incorporation, dissolution, or replacement by this new body of the four major regional health bodies: Office International d’Hygie`ne Publique (OIHP), United Nations Relief and Rehabilitation Administration (UNRRA), League of Nations Health Organization, and the Pan American Health Organization (PAHO). The functions of the OIHP, UNRRA, and the League of Nations Health Organization were taken over by the WHO. The PAHO still stands as a separate international organization; its secretariat, the Pan American Sanitary Bureau (PASB), serves as the regional office of the WHO for the Americas. The name World Health Organization was suggested by Dr. George B. Chisholm, who at the time was the Deputy Minister of National Health of Canada, and eventually became the first Director-General of the WHO (UN WHO interim commission 17) (Table 1).
The constitution of the WHO states its objective as the attainment by all peoples of the highest possible level of health. Health was further defined as a state of physical, mental, and social well-being and not merely the absence of disease or infirmity. Additional entries in its constitution enshrine health as a human right and state its necessity for peaceful living.
Structure
The World Health Organization has 193 member states. Its headquarters is in Geneva, Switzerland, and it maintains six regional offices (for the Americas, Europe, Africa, South-East Asia, Eastern Mediterranean, and Western Pacific) and 148 country or special offices. Membership is granted on acceptance of the WHO constitution for UN member states, or by a simple majority vote of the World Health Assembly (WHA) for other states. Instruments of acceptance of the WHO constitution are deposited with the Secretary General of the UN. The official languages of the WHO are Arabic, Chinese, English, French, Russian, and Spanish.
In line with its status as a global coordinator, the WHO has a complex series of arrangements and agreements with various bodies and governments. It is engaged in partnerships with bodies both within and outside the UN structure (e.g., United Nations Children’s Fund, United Nations Development Program, World Trade Organization, World Bank, the Joint United Nations Program on HIV/AIDS, Gates Foundation, Food and Agriculture Organization, etc.).
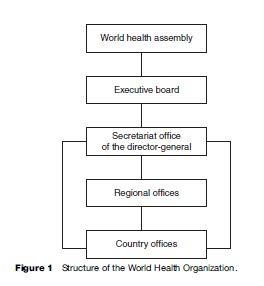
The WHO is functionally decentralized, but three main organs can be identified as stipulated in Article 9 of its constitution (Figure 1): The World Health Assembly, the Executive Board (EB), and the Secretariat.
The World Health Assembly
This is the highest decision-making body of the WHO. It convenes once a year, usually in May, on a date set by the EB. However, special sessions may be convened. It comprises delegations from the member states, and various categories of observers invited by the WHO Director-General (DG). Articles 18 to 23 of the constitution specify the functions of the WHA. Notably, it sets the policy direction for the WHO, appoints the DG, approves the biennial budget, and provides financial oversight.
The Executive Board
The executive board is made up of appointees from 34 member states. Member states eligible to appoint board members are selected by the WHA, and remain so for three years with renewable terms. These appointees serve not as representatives of their individual countries but as individuals with expertise in health matters. The board has regular meetings twice a year, one before the WHA and another immediately after the assembly for administrative matters. One of the board members is elected the chairman of the board for a period of one year. Article 28 of the constitution specifies the functions of the board. Notably it prepares the agenda for the WHA and appoints regional directors following nominations by regional committees. It also nominates a candidate, from individuals put forward by member states, for the post of DG. It serves as the executive arm of the WHO.
The Secretariat
The DG of the WHO is the head of the Secretariat, which comprises all the WHO staff at all levels (headquarters, regional offices, and country or liaison offices). The DG serves as the chief technical and administrative officer. His or her appointment to the post is by the WHA and lasts for a term of five years. The Secretariat is responsible for carrying out WHO activities and administrative functions necessary for the WHA and EB to function. Within the office of the DG there is a Deputy Director-General. All staff worldwide are under the authority of the DG and are granted the privileges of diplomats, in accordance with agreements between the WHO and member states. Credence is given to this arrangement as the WHO is a specialized agency of the UN (WHO, 2007).
Associated with the office of the Director-General are 11 divisions or offices run by Assistant Directors-General, and the regional offices. The divisions are: Health Action in Crises; Information, Evidence and Research; Communicable diseases; Noncommunicable diseases and Mental Health; Family and Community Health; AIDS, Tuberculosis (TB) and Malaria; Health Systems and Services; General Management; Sustainable Development and Healthy Environments; Health Technology and Pharmaceuticals and WHO office at the UN. Within the divisions, there are a varying number of directors. The DG also has special representatives on various issues and links to partner organizations such as the United Nations.
WHO maintains six regional offices, which encompass the country offices. Member states are assigned to regions based on geography, with some political considerations. The regional offices are: Africa (AFRO), Americas (AMRO), Eastern Mediterranean (EMRO), Europe (EURO), South-East Asia (SEARO), and Western Pacific (WPRO). A regional director heads each regional office. A regional committee consisting of representatives of member states in the region sets regional policies and allocates resources based on the budget allocated to the region by the WHA. The freedom to design their own budget gives the regional offices some degree of autonomy. They work toward the overall objectives set by the WHA but also take into account regions’ specific issues. Hence the regions have different organizational structures and priorities.
WHO Regional Office For Africa (AFRO)
Located in Brazzaville, Congo, the AFRO covers 46 countries. The population of the region is approximately 748 million. Maternal and child health, malaria, TB, and HIV/AIDS are high on the agenda with a renewed focus on health systems development and disease surveillance.
WHO Regional Office For The Americas (AMRO)
The PAHO, as previously stated, acts as the regional office for the WHO in the Americas. It also serves as the specialized organ for health in the Inter-American system. It covers 35 countries and is located in Washington, DC, in the United States. Some countries are participating states, associate members, or have observer status in the PAHO even though they belong to other WHO regions. This is because they have sovereign rights to nations within the Americas. The population of the region is approximately 893 million people. Regional concerns include inequities in health care, vaccine coverage, and human resources for health and tobacco control.
WHO Regional Office For The Eastern Mediterranean (EMRO)
Located in Cairo, Egypt, the EMRO covers 21 countries. The population of the region is approximately 557 million people. Priority programs of the office include: the Tobacco Free Initiative, Roll Back Malaria, Stop Malaria, and its community-based initiatives. The Special Program on Polio Eradication reports directly to the regional director.
WHO Regional Office For Europe (EURO)
Located in Copenhagen, Denmark, the EURO covers 53 countries in the region. The population of the region is approximately 888 million. In this region, noncommunicable diseases account for 77% of the burden of disease, and communicable diseases rank third, accounting for 9%. With cardiovascular diseases and cancer the leading conditions, the prevention aspect of the WHO work comes to the fore. Specific programs address risk factors such as smoking, diet, exercise, and air pollution. Mental health is an important issue for the region.
WHO Regional Office For South-East Asia (SEARO)
Located in New Delhi, India, the SEARO covers 11 countries in the region. The population of the region is approximately 1.68 billion people. Reproductive health issues, malaria, leprosy, and a variety of other communicable diseases are high on the agenda in this region.
WHO Regional Office For The Western Pacific (WPRO)
Located in Manila, Philippines, the WPRO covers 27 countries. The population of the region is approximately 1.75 billion people. The regional priorities include new challenges such as emerging infectious diseases – severe acute respiratory syndrome (SARS) and avian influenza – and long-standing concerns such as HIV/AIDS, tobacco control, and health worker migration.
Country offices are headed by WHO representatives, heads of office, or liaison officers. They are appointed by the regional director. These offices form the main structure for cooperation with governments. Only 145 country offices exist, with three special offices: US-Mexican border office, WHO office in Jerusalem, and the office in the UN administrative region of Kosovo. These country offices are responsible for individual countries with some such as those of Barbados, Venezuela, and Samoa covering multiple countries. Thirty-four member states have no country offices, for example, Canada, Ireland, Israel, Malta, San Marino, United Kingdom of Great Britain, United Arab Emirates, Australia, Japan, and the United States. Thirty-two subcountry offices exist. The WHO maintains other offices such as the WHO office at the European Union, the WHO Center for Health Development in Kobe, Japan, and the WHO office at the African Union, but they are not classified as country offices.
Funding
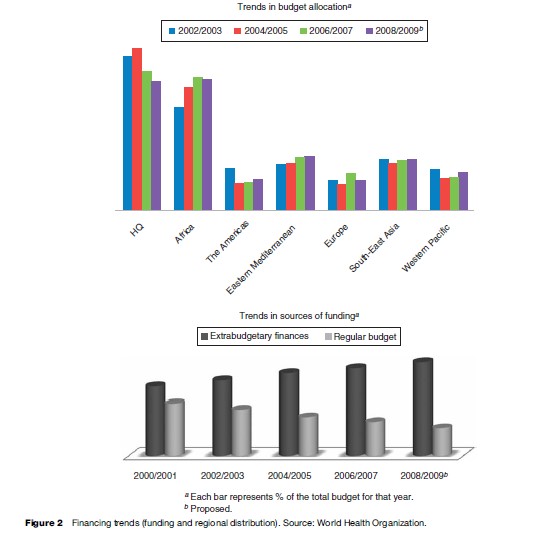
The WHO derives most of its funding from two main sources, obligatory annual contributions from member states and voluntary contributions from the governments of member states and other organizations. The exact amount of obligatory contributions from member states is determined using a formula agreed on by the WHA and constitutes the regular budget. Voluntary contributions from governments and other agencies make up the extra budgetary finances. Extra budgetary finances account for a significant proportion of the operating funds. In 2006/2007, it accounted for approximately 72% of the $3.3 billion budget. In the proposed budget for 2008/2009 this proportion will rise to approximately 77%. Budgets are prepared on a biennial basis by the DG with input from the divisions and regional offices. In the current budgetary cycle 30% of the funds are earmarked for the headquarters and the remaining funds are divided in varying proportions among the regional offices (6% for the Americas, 29% for Africa). This continues the trend of shifting funds to the regions (Figure 2). The DG forwards the final budget proposal for consideration and approval by the EB and ultimately the WHA.
Functions
The WHO, as specified in its constitution, acts as the directing and coordinating authority in international health work and its functions are listed in Article 2 of its constitution. Given the definition of health in the constitution and the inexact phrasing of its functions, its spectrum of activities is very wide. In the Ninth General Program of Work the WHO provides a wordy description of its function and activities, stating
WHO’s directing and coordinating functions include the search for international consensus on health problems of global priority and the most effective ways of assisting countries to solve them, and advocacy of measures to mobilize international resources and action for health, including humanitarian assistance. They also comprise what is often referred to as normative function of WHO, that is, monitoring the health situation and trends throughout the world; proposing conventions, regulations, norms, standards and guidelines related to health; and stimulating research, the advancement and application of knowledge, and the sharing of information in the field, including the bioethical dimensions’(WHO 1994: 23–24).
Periodically the WHO approves a general program of work (GPW) that further defines the long-term policy direction of the organization, the six-year medium-term strategic plan, and the biennial budget providing short-term direction. In its 11th General Program of Work, covering 2006–2015, six core functions are highlighted (WHO 2006: 25–30):
- Providing leadership on matters critical to health and engaging in partnerships in which joint action is needed.
- Shaping the research agenda and stimulating the generation, translation, and dissemination of valuable knowledge.
- Setting norms and standards, and promoting and monitoring their implementation.
- Articulating ethical and evidence-based policy options.
- Providing technical support, catalyzing change, and building sustainable institutional capacity.
- Monitoring the health situation and assessing health trends.
This GPW incorporates attainment of the health-related aspects of the Millennium Development Goals to a greater degree than previous programs.
Programs
The precise scope of the functions of the WHO is open to interpretation. A brief look at some of their actual activities and achievements may provide a better perspective of its role. The WHO attempts to achieve its objectives in a variety of ways, collaborating with states, intergovernmental institutions, nongovernmental institutions, and engaging in public–private sector partnerships. They have designated numerous institutes as collaborating centers involved in various projects. They also raise expert committees and advisory panels to ensure expertise in addressing the wide spectrum of issues that fall under its bailiwick. The annual World Health Reports have raised awareness of issues such as gaps in access to health care (1995), noncommunicable diseases (1997), health systems performance (2000), mental health (2001), and human resources for health (2006). They have offices or commissions focused on social determinants of health; child and adolescent health and development; macroeconomics and health; gender, women, and health; intellectual property rights, innovation, and public health; disability and rehabilitation; blood transfusion safety; and globalization of trade and health. Initiatives launched include 3 by 5, Civil Society Initiative, the Burden of Disease project, Global Campaign for Violence Prevention, and the International Medical Products Anti-Counterfeiting Task Force. The WHO uses high-profile individuals to raise awareness of significant health issues by designating them goodwill ambassadors on a yearly basis. They also designate specific days of the year to highlight specific health problems, for example, 24 March – World TB Day, 1 December – World AIDS Day, and 14 November – World Diabetes Day.
A few notable achievements of the WHO include the preparation and periodic revision of the International Classification of Diseases (ICD) under the WHO Family of International Classifications (WHO-FIC); the ‘Health for All’ initiative launched in Almaty (formerly Alma-ata), Kazakhstan (1978); the eradication of smallpox (1979), an international code on the marketing of breast milk substitutes (1981); the global strategy on diet, physical activity, and health (2004); a review of international health regulations (2005); the Framework convention on tobacco control (2005); and the push for the eradication of polio. The role of the WHO in facilitating research should not be neglected: in league with its collaborating centers it has made advances in the development of antimalarial drugs, vaccines, anti-TB drugs, and the provision of uniform treatment guidelines for various conditions such as diarrhea and malaria.
In 2003, the late DG of the WHO, Dr. Lee Jong-wook said, ‘‘We must do the right things. We must do them in the right places. And we must do them the right way. We are putting countries where they should be – at the heart of WHO’s work’’ (Lee 2003). This voices the importance and necessity of the WHO country policy. The WHO provides country-level support through its country offices in the form of policy recommendations and technical assistance in dealing with potential and existing public health threats. A recent example of the effectiveness of the WHO was seen in 2003 with the containment of a potential SARS outbreak and the tracking and containment of the spread of avian influenza.
WHO is the administrator of a number of foundations; a function either inherited from the League of Nations Health Organization or designated so since its inception. They include the Darling Foundation, the Le´on Bernard Foundation, the Dr. A. T. Shousha Prize and Fellowship, and the Jacques Parisot Foundation Fellowship.
Publications
The WHO library information system (WHOLIS) maintains a collection of all WHO publications and releases. The WHO statistical information database (WHOSIS) maintains records detailing global health statistics. The WHO headquarters and its regional and country offices publish a number of journals, books, pamphlets, and handbooks.
The premier publication of the WHO is the World Health Report. First published in 1995 and released annually on World Health Day, each edition is dedicated to a specific theme. Its publication generates countless research articles and discussions related to the highlighted theme, effectively putting it on the world agenda. The regional offices release regional health reports describing the health situations in their regions and their efforts to improve them. Periodicals released by the WHO or its regional offices include the Bulletin of the World Health Organization, Weekly Epidemiological Record, WHO Drug Information, Eastern Mediterranean Health Journal, and the Pan American Journal of Health.
The WHO Technical Report series contains the final reports of expert committees or working groups appointed by the WHO to examine specific issues. Other publications from the WHO are released sporadically to highlight issues and provide guidance to the public health community, for example, ‘TB/HIV: A Clinical Manual’; ‘Pathology and Genetic Tumors of the Skin’; ‘Basic Epidemiology’; and ‘Building Better Health: A Behavioral Change and Essentials for Emergencies.’ The WHO Press is the main publisher of WHO materials. Their publications have won a number of awards.
Challenges And Prospects
Some of the achievements of the WHO have been highlighted, but this by no means reduces the daunting task facing the organization. In a world with a population of over 6 billion, more that double that in 1948, the WHO is more important than ever. Its definition of health envisaged a role beyond disease prevention and cure, although these remain the most visible aspects of its activities. WHO activities cover a wider spectrum with programs like WHO-CHOosing Interventions that are Cost Effective (WHO-CHOICE). This program assists member states in setting priorities and identifying cost-effective interventions by assembling regional data on costs and health implications of interventions. Another example is the International Clinical Trial Registry Platform, which, while not an administrative register, aims to establish ethical standards for trials involving humans. They hope to create minimum standards for reporting these trials and make this information readily available to interested parties.
In some ways the organization is a victim of its own success; prolonged life expectancy has come with an increasingly aged population. This poses a challenge to health systems in terms of shifting the burden of disease and sustainability. Disease surveillance is carried out in an increasingly political environment. There is an added urgency in detecting new and old infectious diseases as global travel has enhanced the speed and range of their possible spread.
The WHO activities have not been without controversy, from initial opposition to its attempts to promote breast milk over formula feeds to the much derided ranking of national health systems performance in the World Health Report of 2000, it has sparked debate on the issues. However, failures to achieve its target on polio eradication and provision of AIDS medications also serve as reminders of the organization’s fallibility.
Tropical Diseases
An in-depth look at the fight against tropical diseases shows how the agency has had to reinvent itself and reach out to achieve its objectives. To start with, it is worthwhile pointing out that the term tropical disease as commonly used is a misnomer. It is used to refer to conditions with a high prevalence in the tropics, or those classified as less-developed countries. This includes not only conditions exclusive to the tropics, the true meaning of the term, but also conditions that have largely been controlled in first-world nations. Thus, tropical disease treatment refers to efforts to alleviate the burden posed by mostly infectious conditions that constitute a high burden of disease in the developing world.
In 1975, the WHO, the UN Children’s Fund (UNICEF), the UN Development Program, and the World Bank established the Special Program for Research and Training in Tropical Diseases (TDR). It aims to combat a portfolio of major diseases of the poor and disadvantaged. Working in collaboration with research labs and governments it uses two broad approaches to achieve its aims: fostering research and development focused on problems in endemic areas, and training and strengthening capacity in endemic countries to facilitate further research and implementation.
Since then, the WHO has entered into other alliances with various organizations in an attempt to control tropical diseases. Within the structure of the WHO, a division headed by an assistant director-general is devoted to HIV/AIDS, TB, and malaria. Different programs, alliances, and initiatives focus on tropical diseases. Some of them include the Global Task Force on Cholera Control established in 1992; the International Guinea Worm Eradication Program spearheaded by The Carter Center in collaboration with WHO, UNICEF, and others launched in 1996; the WHO Alliance for the Elimination of Blinding Trachoma by 2020 (GET2020) launched in 1997; the Global Buruli Ulcer Initiative (GBUI) established in 1998; the Roll Back Malaria partnership (RBM) launched in 1998; the Stop TB partnership endorsed by the WHA in 2000; and the Global Alliance to Eliminate Lymphatic Filariasis launched in 2000.
These programs and initiatives have resulted in numerous publications and recommendations, for example, the reemergence of indoor residual spraying (IRS) with dichloro-diphenyl-trichloroethane (DDT) and insecticides as a control program, the guidelines on the treatment of malaria, and the guidelines on the treatment of diarrheal diseases.
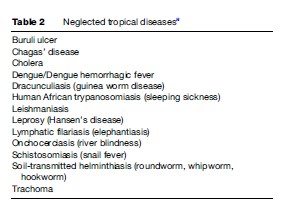
In 2004 and 2005, the WHO developed a conceptual framework for disease control that has been brought to bear in the newly established Department of Neglected Tropical Diseases (NTD). This framework shifts emphasis from a condition-specific approach to addressing the conditions as a group. It has a three-pronged approach consisting of broader coverage with rapid impact interventions, strengthened vector control, and improved surveillance and high-quality care. The department is currently focused on the 13 conditions classified as neglected tropical diseases (Table 2).
The department’s operations are divided into four sections. The first of these, Disease Control in Humanitarian Emergencies, works in association with the Communicable Disease Working Group on Emergencies. The second section, Vector Ecology and Management, focuses on developing evidence-based strategies and providing technical support to interested parties in the area of control of vector-borne conditions. The third and fourth sections function in similar ways, engaging in research and providing technical support, but are distinguished based on three characteristics: availability of effective chemotherapeutic agents, intervention strategies available, and degree of implementation of these strategies. The third section, Preventive Chemotherapy and Transmission Control, deals with conditions for which effective chemotherapeutic agents and cost-effective intervention strategies exist. Thus, their focus is on the widespread implementation of these strategies. The fourth section, Innovative and Intensified Disease Management, is involved with conditions for which chemotherapeutic agents are available, but for which cost-effective strategies have yet to be developed and implementation of strategies that do exist is minimal. Thus, the department focuses on refining existing strategies and increasing implementation of the best available strategies.
In 2006, the department joined a coalition of international partnerships to form the Global Network for Neglected Tropical Disease Control (GNNTDC). With an estimated 1 billion people suffering from one of these conditions, the implications of continued ignorance are apparent. In partnership with other international bodies aimed at eliminating these conditions, national governments (e.g., Tanzania, Uganda, Mali, etc.), and institutes such as the Albert B. Sabin Vaccine Institute and the Earth Institute, the GNNTDC hopes to avert these consequences. Its initial focus is on five of the neglected tropical diseases (trachoma, soil-transmitted helminthiasis, lymphatic filariasis, schistosomiasis, and onchocerciasis). They are also exploring the negative impact of these conditions on the severity of malaria cases, and susceptibility to HIV/AIDS and TB infection.
In a follow-up to this unified approach, the WHO, as represented in the GNNTDC, has partnered with 24 other agencies to translate these guidelines into policy initiatives by making the materials necessary for the implementation available. The current focus of this new partnership is on the provision of chemotherapeutic agents effective in the prevention of a broad range of diseases caused by worm infestation.
Since their inception, these intervention programs have shown varying levels of success in real terms. Major, significant accomplishments include:
- The elimination of leprosy as a public health problem in 116 of the 122 endemic countries over the last 20 years.
- A decrease in guinea worm cases from 3.5 million in 20 countries in 1985 to 10 000 in 9 endemic countries in 2005.
- Elimination of onchocerciasis as a public health problem in ten West African countries.
- A reduction in the prevalence of sleeping sickness from 300 000 cases in 1995 to between 50 000–70 000 cases currently.
- GET2020 has set 2020 as the target date for the elimination of trachoma, in its 11th GPW, WHO targets 2015 as the date for the elimination of Chagas’ disease.
Conclusion
The peculiar challenges have molded the current shape and direction of the agency as it seeks to maintain its comparative advantage. Margaret Chan, the current WHO DG, in response to a question by The Lancet on the role of the WHO today, said ‘‘No other international or national agency can get to an outbreak scene within 24 hours’’ (Brown 2006). This holds true for many parts of the world. Successive directors-general have navigated the shifting global political terrain and engaged in necessary reforms to the WHO system, streamlining budgetary processes, eliminating redundancy, and creating better cohesion toward achieving policy objectives. While still a work in progress, the recognition of the need for the WHO is the first step in a journey of a thousand miles.
Bibliography:
- Brown H (2006) WHO’s Director-General candidates respond. The Lancet 368: 1225–1228.
- Lee JW (2003) Address to WHO staff on 21 July 2003. https://www.who.int/dg/lee/speeches/2003/21_07/en/
- United Nations World Health Organization Interim Commission (1947). Official records of the World Health Organization No 1: Minutes of the technical preparatory committee for the International Health Conference held in Paris from 18 March to 5 April 1946. Geneva, Switzerland: United Nations World Health Organization.
- World Health Organization (WHO) (1994) Ninth General Program of Work (1996–2001), pp. 23–24. . Geneva, Switzerland: WHO.
- World Health Organization (WHO) (2006) Engaging for health. Eleventh General Program of Work 2006–2015. A Global Health Agenda. Geneva, Switzerland: WHO.
- World Health Organization (WHO) (2006) Neglected Tropical Diseases: Hidden Successes, Emerging Opportunities. Geneva, Switzerland: WHO.
- Burci GL and Vignes C (2004) World Health Organization. The Hague, The Netherlands: Kluwer Law International.
- Minelli E (2003) World Health Organization: The mandate of a specialized agency of the United Nations. Dissertation for the Political Science Degree specializing in International Institutions at the Catholic University of Milun in association with the WHO collaborating Centre for Traditional Medicine, University of Milan.
- World Health Organization (WHO) (2007) Working for health: An introduction to the World Health Organization. Geneva, Switzerland: WHO Press.
- World Health Organization (WHO) (2006) Engaging for Health. Eleventh General Program of Work 2006–2015. A Global Health Agenda. Geneva, Switzerland: WHO.
- World Health Organization (WHO) (2006) A Guide to WHO’s Role in Sector Wide Approaches to Health Development. Geneva, Switzerland: WHO.
- World Health Organization (WHO) (2005) WHO Country Cooperation Strategies. A Guiding Framework. Geneva, Switzerland: WHO.
- World Health Organization (WHO) (2006) Neglected Tropical Diseases: Hidden Successes. Emerging Opportunities. Geneva, Switzerland: WHO.
- World Health Organization (WHO) The Constitution of the World Health Organization. Geneva, Switzerland: WHO.
- https://www.who.int/ – World Health Organization.
ORDER HIGH QUALITY CUSTOM PAPER

Always on-time

Plagiarism-Free

100% Confidentiality