
Sample Epilepsy Research Paper. Browse other research paper examples and check the list of research paper topics for more inspiration. If you need a research paper written according to all the academic standards, you can always turn to our experienced writers for help. This is how your paper can get an A! Also, chech our custom research proposal writing service for professional assistance. We offer high-quality assignments for reasonable rates.
Epilepsy is a common disorder of the central nervous system (CNS) characterized by recurrent seizures. Seizures come in a variety of forms—some primarily motor and some affecting consciousness; some restricted to a local brain region and some involving the entire brain; some so dramatic as to be frightening and some so subtle as to be easily missed by the casual observer (Engel 1989, Engel and Pedley 1998). Current estimates are that approximately 1 percent of the population has a seizure disorder. Epilepsy respects no national, racial, or ethnic boundaries. Thirty to fifty percent of epilepsies in the U.S. (and other medically ‘sophisticated’ countries) are inadequately controlled by medication; that percentage is much higher in underdeveloped nations. Better understanding of the bases of seizure disorders is critical if we are to develop more effective treatments—and cures. This research paper provides a brief overview of our current insights into the cellular and molecular causes of epilepsy, and identifies the challenges for epilepsy research.
Academic Writing, Editing, Proofreading, And Problem Solving Services
Get 10% OFF with 24START discount code
1. Definition Of Terms
Although the term ‘epilepsy’ is usually used in the singular, ‘epilepsy’ (like ‘cancer’) refers to a diverse set of abnormalities, with different causes and different clinical expressions. The epilepsies are defined as chronic seizure conditions, and categorized by clinicians on the basis of the characteristic behavior and associated pattern of brain electrical discharge (the electroencephalogram, or EEG). This categorization scheme (Commission on Classification and Terminology of the International League Against Epilepsy 1981, 1989) has resulted in a useful—although complex—system for diagnosis and treatment, but generally ignores the underlying bases (molecular and cellular) for the seizures. A seizure can be viewed as a paroxysmal and synchronous discharge of a large population of neurons. Occurrence of an isolated, single seizure does not necessarily reflect brain pathology. Indeed, seizures can occur in the normal brain, and reflect normal responses to stress or injury. Repetitive seizures, however, signal some chronic pathological condition of the CNS. Understanding that abnormality has been particularly difficult because the symptom—the seizure—is (for most epilepsies) episodic and unpredictable. Further, during the time between seizures (which may be months, or even years), the brain functions in an apparently normal fashion. Indeed, it is the unpredictability of seizures— as well as the loss of voluntary controls during these ‘ictal’ (i.e., seizure) episodes—that constitute major contributors to the morbidity associated with epilepsy.
2. Categorization Of Epilepsy Syndromes
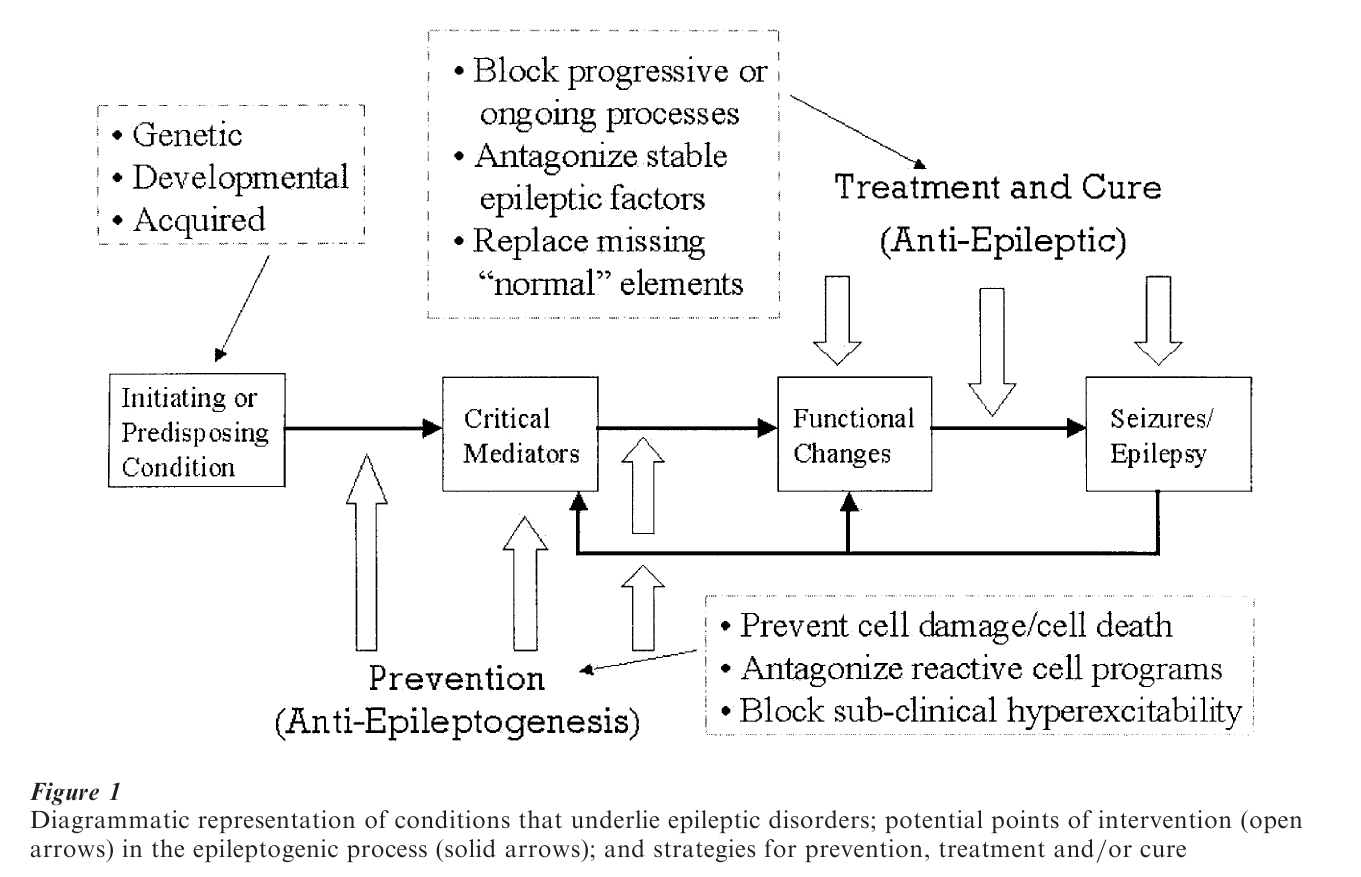
With advances in our understanding of underlying mechanisms of seizures, and of the processes by which a chronic seizure state is acquired (i.e., ‘epileptogenesis’), it is now possible to categorize many epileptic disorders on the basis of the neurobiological cause rather than simply on the basis of the seizure behavior and EEG pattern. A general classification scheme, that covers most epilepsies, includes the following (overlapping) three categories: genetic disorders; developmental disorders; and acquired epilepsies (Fig. 1).
2.1 Genetic Disorders
A number of epilepsies have now been traced to single gene mutations. Many of the implicated genes code for ion channels (e.g., for sodium, potassium, or calcium) or for neurotransmitter receptor proteins (e.g., for acetylcholine or gamma-aminobutyric acid) (Berkovic and Scheffer 1999). Abnormalities in these proteins make at least some intuitive ‘sense’ in trying to understand seizure discharge, for much is known about how ion flux and neurotransmitters affect brain excitability. Other ‘epilepsy genes’ have been associated with structural brain abnormalities, such as seen in lissencephaly or tuberous sclerosis (Spreafico et al. 1999); abnormalities in these gene products result in developmental disorders generated through molecular signaling aberrations that we are just beginning to understand. Some of the implicated genes have functions yet to be elucidated. While single gene epilepsies are relatively rare, it is clear than some of the more common epilepsies (for example, childhood absence epilepsy—CAE, or juvenile myoclonic epilepsy—JME) are inherited in a more complex fashion, suggesting that multiple genes play roles in these disorders. Genetics also appears to play a significant role in determining seizure susceptibility, even in the normal population. Thus, major challenges for the field include characterizing and identifying the genes involved in multigenic seizure disorders, and gaining a better understanding of which genes are important in determining seizure predisposition. In addition, it is critical to understand the cellular pathways through which these genic abnormalities lead to neurophysiologic dysfunction. Identifying ‘epilepsy genes’ is not enough to solve the mystery of aberrant function. It is, however, a critical start— especially useful in developing new drugs (or other treatments) with specific molecular targets.
2.2 Developmental Disorders
The process of brain development is marvelously complex. Developmental neuroscience research has provided a rich background regarding the genetic and molecular signals involved in constructing a normal mammalian brain (Sanes et al. 2000). Abnormalities in these processes—in cell proliferation, migration, differentiation, and establishment of connections—may all lead to neurological disorders, including epilepsy (Schwartzkroin et al. 1995). Given the potential for developmental mistakes, it is actually quite remarkable that the incidence of neurological dysfunction is as low as it is. It should come as little surprise that seizure occurrence is higher among children (estimated at approximately 4 percent) than in the adult population—partly as a result of abnormalities in brain development (Spreafico et al. 1999), and partly because the properties of the immature brain render it particularly seizure-prone (Nehlig et al. 1999). The epilepsy incidence in children with other developmental disorders—cerebral palsy, mental retardation, autism, fragile X syndrome, etc.—is perhaps 10 times that in otherwise normal children, undoubtedly reflecting a general underlying brain pathology (Dodson and Pellock 2000). Since seizure incidence is so high among the young, since epilepsies may reflect abnormalities of genetics and/or brain development, and since the brain is so vulnerable to perinatal trauma (e.g., hypoxia, head trauma, infection), many epileptologists consider epilepsy to be primarily a set of disorders of childhood (Schwartzkroin and Moshe 2000). Why is it that these early insults are so likely to induce an epileptic state? Why do developmental brain abnormalities, such as seen in tuberous sclerosis or various forms of lissencephaly, correlate so highly with early seizure syndromes? We are just beginning to get a glimpse of the answers to these questions—and the general theme seems to revolve around the highly ‘plastic’ nature of the immature CNS. While in the adult, brain trauma often leads to cell death and loss of function, the immature brain is more resilient. Immature neurons appear to be less sensitive to injurious stimuli. The immature brain is capable of producing new neurons to a much greater extent than is the adult CNS. Immature nerve cells more readily make new connections when normal organization of the system is disrupted. While this ‘plasticity’ preserves a significant amount of behavioral function, it may come at a cost—for the new circuits established by injured neural elements may not be entirely normal. Marginal injury and inappropriate connections appear to be two major contributors to the development of abnormal electrical activity—i.e., seizures.
2.3 Acquired Epilepsies
Many epilepsies can be associated with a particular traumatic stimulus (e.g., head injury) or medical condition (e.g., a tumor or an infection), and thus are designated ‘acquired.’ The implication of this designation is that the brain is (was) otherwise normal, and that the identified insult is the sole cause for the epilepsy. This assumption allows us to examine the variables associated with the epileptic condition, and thus to better understand what mechanisms are responsible for development of the epileptic state. As suggested above, many of our current hypotheses revolve around the new connections made by the injured brain, and the loss of critical elements that control the electrical excitability of the system. However, while it may well be the case that a given traumatic stimulus is the critical ‘trigger’ for epileptogenesis, it remains something of a mystery why such injury in one individual will lead to an epileptic state but the same injury to another individual will not. This situation has led to the concept of ‘predisposition’ with respect to epileptogenesis (Fig. 1). That is, there may be subtle factors—gene-based differences in seizure susceptibility, subclinical injury, or developmental abnormalities—that provide a background upon which a brain insult plays out. A subtle, preexisting injury may make it more likely that an individual with head trauma develops epilepsy at a later time. This concept also implicates another important possibility that is often discussed, especially within the context of pediatric epilepsies—that epilepsy is a ‘progressive’ disorder (Heinemann et al. 1996, Engel et al. 2000), which develops as a result of active neuronal processes. Thus, an initial subtle and benign insult may ‘kindle’ into a more significant and clinically troubling condition over months, or even years.
3. Basic Neuronal Mechanisms Underlying Seizure Discharge
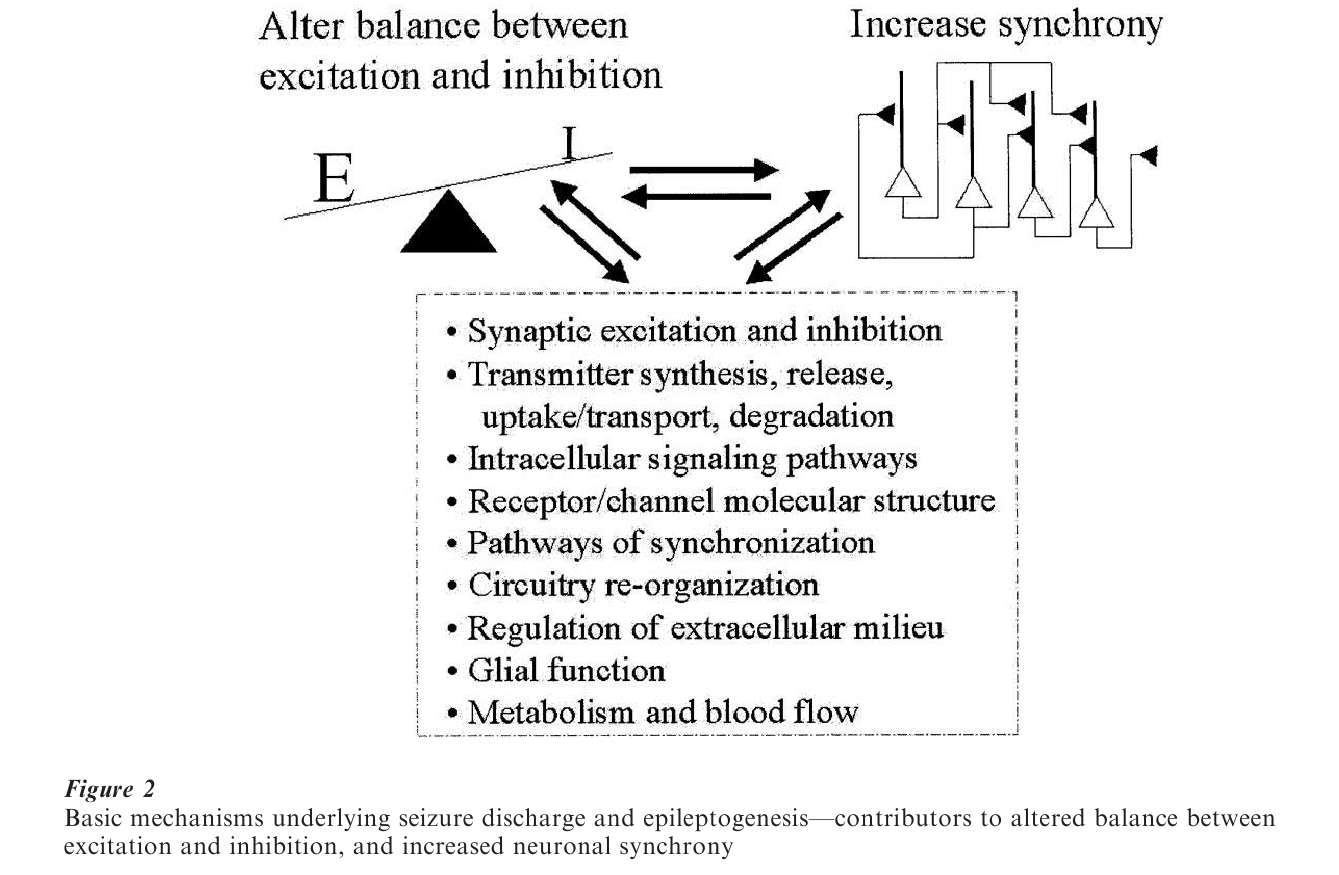
In general, it is thought that seizures arise as a result of an imbalance between the processes responsible for excitation and inhibition in the brain (Fig. 2). This imbalance leads not only to a state of ‘hyperexcitability’ but also to a condition of ‘hypersynchrony’; that is, the neurons discharge at a higher rate than normally, and discharge in a characteristically synchronous pattern that overrides the normal patterns of neuronal activity. There are a host of processes to consider in trying to understand these changes (Fig. 2) (Delgado-Escueta et al. 1996). Most research has focused on the mechanism through which nerve cells generate electrical activity (i.e., the ionic balance and ion-selective channels that are the basis for neuronal signaling) and the neurochemical communication systems through which neurons excite or inhibit each other. These are the basic neurophysiological ‘building-blocks’ of brain function, critical to any consideration of neural activity, in the normal brain as well as in the brain exhibiting a neurological disorder. Indeed, investigations to understand the basic mechanisms of the epilepsies have contributed greatly to our understanding of normal brain function, and to dysfunction in other neurological pathologies.
The excitation–inhibition balance in normal brain is delicately regulated—perhaps to allow for the maximum degree of ‘plasticity’. While excitatory discharge is a sign by which we recognize neuronal electrical activity, it is the inhibition that sculpts the patterns of interaction that make up normal information processing. Thus, much of epilepsy research has focused on key inhibitory mechanisms, and many theories regarding underlying epileptic processes involve changes in the quantity—or quality—of inhibitory mechanisms. A key to much of this analysis is the critical role played by the predominant inhibitory neurochemical in the forebrain, gamma-aminobutyric acid (GABA). Reduction of GABA synthesis, loss or reorganization of neurons that use GABA for their neurotransmission, and/or alterations in the receptors sensitive to this molecule have all been proposed as mechanisms of epilepsy. Also noteworthy is the fact that many of the antiepileptic drugs currently in use exert their actions, at least in part, through GABA receptors. It is clear that even small changes in this inhibitory system can have serious consequences. For example, blocking only 15–20 percent of GABA receptors can, in experimental preparations, produce seizures. Thus, in elucidating underlying seizure mechanisms, we are faced not only with identifying the salient processes, but also understanding the significance of mechanistic disruption in quantitative terms.
Basic epilepsy research since the 1960s has focused on the cellular and molecular mechanisms responsible for seizure activity. We have still to approach the bigger question of how a chronic seizure state is established. Research into the basic mechanisms of epileptogenesis is now a priority in many laboratories, in large measure because investigators see an opportunity to ‘cure’ epilepsy before it starts (Fig. 1). An important goal is to identify/diagnose ‘at risk’ patients, and treat them so as to disrupt the underlying processes of epilepsy development. Much of this research is driven by the idea that epilepsy development ‘recapitulates’—at least in some important processes—early developmental processes. Thus, there is much interest in the signaling molecules that guide the development of neuronal connections and of mature electrophysiological properties. Indeed, it is the plasticity of these processes, even in the adult brain, that have become primary targets in research and in treatment development.
4. Epilepsy And Brain Plasticity
What are the ‘plastic’ processes that give rise to epileptic conditions? As suggested above, many investigators believe that they are the same processes that we have identified as the basis for higher brain functions, such as learning and memory. We can define ‘plasticity’ as the ability of the brain to respond (structurally and/or functionally) to new stimuli, with adaptive behavior. Such plasticity is one of the primary functions of the highly developed cortical regions of the mammalian brain, where we believe that learning takes place—and where (perhaps not coincidentally) most seizures are generated. Investigators have elucidated many processes that are involved in such complex neural function, including: long-term potentiation (and depression) of synaptic interactions; sprouting of new connections; changes in the number and subunit composition of receptors and channels; proliferation and/or death of neural and glial elements; and (of course) the up(or down-) regulation of the genes that code for protein products involved in these changes (Fig. 2) (Engel et al. 2000). These are all normal brain mechanisms. They are all implicated in genesis of epileptic conditions. The epileptic state is characterized by a loss of regulation or control of these plasticities. A little plasticity is critical for higher brain function, but too much plasticity leads to pathology.
Bibliography:
- Berkovic S F, Scheffer I E 1999 Genetics of the epilepsies. Current Opinions in Neurology 12: 177–82
- Commission on Classification and Terminology of the International League Against Epilepsy 1981 Proposal for revised clinical and electroencephalographic classification of epileptic seizures. Epilepsia 22: 489–501
- Commission on Classification and Terminology of the International League Against Epilepsy 1989 Proposal for revised classification of epilepsies and epileptic syndromes. Epilepsia 30: 389–99
- Delgado-Escueta A V, Wilson W A, Olsen R W, Porter R J (eds.) 1986 Jasper’s Basic Mechanisms of the Epilepsies, 3rd edn. Lippincott Williams & Wilkins, Philadelphia
- Dodson W E, Pellock J M (eds.) 2000 Pediatric Epilepsy, Diagnosis and Therapy, 2nd edn. Demos, New York
- Engel J Jr 1989 Seizures and Epilepsy. F.A. Davis, Philadelphia
- Engel J Jr, Pedley T A (eds.) 1998 Epilepsy: A Comprehensive Textbook. Lippincott-Raven, Philadelphia
- Engel J Jr, Schwartzkroin P A, Moshe S L, Lowenstein D H (eds.) 2000 Brain Plasticity and Epilepsy. Academic Press, San Diego
- Heinemann U, Engel J Jr, Avanzini A, Meldrum B S, Mouritzen-Dam A, Wasterlain C (eds.) 1996 Progressive Nature of Epileptogenesis. Elsevier, Amsterdam
- Nehlig A, Motte J, Moshe S L, Plouin P (eds.) 1999 Childhood Epilepsies and Brain Development. John Libbey, London
- Sanes D H, Reh T A, Harris W A 2000 Development of the Nervous System. Academic Press, New York
- Schwartzkroin P A, Moshe S L (eds.) 2000 Pediatric epilepsy. Mental Retardation and Developmental Disabilities Research Reviews 6(4)
- Schwartzkroin PA, Moshe S L, Noebels J L, Swann J W (eds.) 1995 Brain Development and Epilepsy. Oxford University Press, New York
- Spreafico R, Avanzini G, Andermann F (eds.) 1999 Abnormal Cortical Development and Epilepsy. John Libbey, London
ORDER HIGH QUALITY CUSTOM PAPER

Always on-time

Plagiarism-Free

100% Confidentiality