
Sample Psychosocial Theories Of Health Behavior Research Paper. Browse other research paper examples and check the list of research paper topics for more inspiration. If you need a research paper written according to all the academic standards, you can always turn to our experienced writers for help. This is how your paper can get an A! Feel free to contact our custom research paper writing service for professional assistance. We offer high-quality assignments for reasonable rates.
The term ‘health behavior’ is used very broadly in this research paper to refer to any behavior that influences, or is believed to influence, physical health outcomes, either by increasing or decreasing their risk or severity. A number of psychosocial theories (or models—the two terms are used interchangeably in this research paper) has been developed to predict, explain, and change such health behaviors. These theories can be divided into two main groups which are commonly referred to as social cognition models and stage models, respectively. These are discussed in turn.
Academic Writing, Editing, Proofreading, And Problem Solving Services
Get 10% OFF with 24START discount code
1. Social Cognition Models
The term ‘social cognition models’ is used to refer to a group of similar theories, each of which specifies a small number of cognitive and affective factors (‘beliefs and attitudes’) as the proximal determinants of behavior. These models do not deny that behavior is influenced by many other factors (e.g., social structural, cultural, and personality factors), but they assume that the effects of such distal factors are largely or completely mediated by the proximal factors specified by the model. Unlike the distal factors, the proximal factors are assumed to be amenable to change, for example by provision of relevant information. Thus social cognition models can be used as the basis for health behavior interventions.
The five models that have been used most widely by health behavior researchers in recent years are shown in Fig. 1 in the form of causal diagrams. The diagrams depict the core constructs in each model; numerous variations appear in the literature.
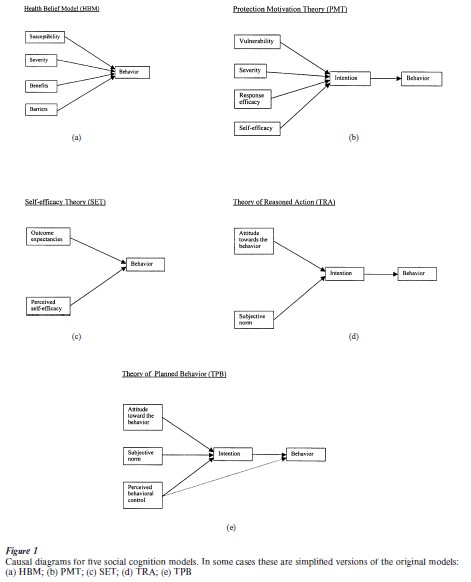
1.1 The Health Belief Model
The health belief model (HBM; Becker 1974) was developed in the 1950s by a group of social psychologists working in the field of public health who were seeking to explain why some people do not use health services such as immunization and screening. The model is still in common use. There are four core constructs: the first two refer to a particular disease whereas the second two refer to a possible course of action that may reduce the risk or severity of that disease. Perceived susceptibility (or perceived vulnerability) is the individual’s perceived risk of contracting the disease if he or she were to continue with the current course of action. Perceived severity refers to the seriousness of the disease and its consequences as perceived by the individual. Perceived benefits refer to the perceived advantages of the alternative course of action including the extent to which it reduces the risk of the disease or the severity of its consequences. Perceived barriers (or perceived costs) refers to the perceived disadvantages of adopting the recommended action as well as perceived obstacles that may prevent or hinder its successful performance. These factors are commonly assumed to combine additively to influence the likelihood of performing the behavior. Thus, high susceptibility, high severity, high benefits and low barriers are assumed to lead to a high probability of adopting the recommended action. Another factor that is frequently mentioned in connection with the HBM is cues to action (events that trigger behavior), but little empirical work has been conducted on this construct.
There have been two meta-analyses (quantitative reviews) of research using the HBM. Janz and Becker (1984) calculated significance ratios showing how often each HBM construct was statistically significant in the predicted direction across 46 studies. These ratios were 81 percent for susceptibility, 65 percent for severity, 78 percent for benefits, and 89 percent for barriers; the pattern of findings was similar when only the prospective studies were examined. Thus, barriers is the most consistent predictor of behavior and severity is the least consistent. Harrison et al. (1992) used extremely strict inclusion criteria; they included only 16 of the 234 studies they originally identified. Across these 16 studies, the mean correlations between HBM components and behavior were 0.15, 0.08, 0.13, and 0.21 for susceptibility, severity, benefits, and barriers, respectively. While statistically significant, these correlations are small in substantive terms. Harrison et al. found that benefits and barriers had significantly larger effect sizes in prospective compared with retrospective studies, whereas severity had a significantly larger effect size in retrospective studies.
1.2 Protection Motivation Theory
Protection motivation theory (PMT; Rogers 1983) was originally developed to explain how people respond to fear-arousing health threat communications or ‘fear appeals.’ It can be regarded as an adaptation of the HBM. Protection motivation refers to the motivation to protect oneself against a health threat; it is usually defined operationally as the intention to adopt the recommended action. Of the determinants of intention specified by the model, the four that have received the most empirical attention are vulnerability and severity (equivalent to perceived susceptibility and severity in the HBM), response efficacy (the belief that the recommended action is effective in reducing the threat), and perceived self-efficacy (the belief that one can successfully perform the recommended action; Bandura 1997). Thus, a person will be more motivated to protect himself or herself (i.e., have a stronger intention to adopt the recommended action) to the extent that he or she believes that the threat is likely if the current course of action is continued, that the consequences will be serious if the threat occurs, that the recommended action is effective in reducing the likelihood or the severity of the threat, and that he or she is able to carry out the recommended action.
In many studies using this model (e.g., Wurtele and Maddux 1987), specific PMT variables are experimentally manipulated in a factorial design and their effects on intention (and sometimes behavior) are measured. In fact, PMT is unique among social cognition models with respect to the relatively large number of experimental tests that have been conducted.
To date, two meta-analyses of PMT studies have been conducted (Floyd et al. 2000, Milne et al. 2000). The analyses used different study inclusion criteria and different effect size measures. Floyd et al. analyzed 65 studies with about 30,000 research participants whereas Milne and colleagues included 27 studies with about 8,000 participants. There were only 12 studies in common. Both analyses found support for each of the main PMT variables as predictors of intentions and/or behavior. Self-efficacy had the strongest, most consistent, and most robust effect.
1.3 Self-Efficacy Theory
Self-efficacy theory (SET) is a subset of Bandura’s (1986) social cognitive theory. According to this approach, the two key determinants of behavior are perceived self-efficacy and outcome expectancies. The latter construct refers to the perceived positive and negative consequences of performing the behavior. See Schwarzer and Fuchs (1996) for a version of this model that incorporates risk perceptions and behavioral intention, as well as components of the action phase of behavior change. No meta-analysis of SET has been published, though there is substantial evidence for the predictive validity of self-efficacy (Schwarzer and Fuchs 1996).
1.4 The Theory Of Reasoned Action And The Theory Of Planned Behavior
The theory of reasoned action (TRA; Ajzen and Fishbein 1980) developed out of social–psychological research on attitudes and the attitude–behavior relationship. The model assumes that most behaviors of social relevance (including health behaviors) are under volitional control, and that a person’s intention to perform a behavior is both the immediate determinant and the single best predictor of that behavior. Intention in turn is held to be a function of two basic determinants: attitude towards the behavior (the person’s overall evaluation of performing the behavior) and subjective norm (the perceived expectations of important others with regard to the individual performing the behavior in question). Generally speaking, people will have strong intentions to perform a given action if they evaluate it positively and if they believe that important others think they should perform it. The relative importance of the two factors may vary across behaviors and populations.
Although not shown in Fig. 1, the TRA also specifies the determinants of attitude and subjective norm. Attitude is held to reflect the person’s salient behavioral beliefs concerning the possible personal con- sequences of the action. For example, a person who believes that performing a given behavior will lead to mostly positive personal consequences will hold a favorable attitude towards the behavior. Specifically, attitude is held to be a function of the sum of the person’s salient behavioral beliefs concerning the outcome of the action each weighted by their evaluation of that outcome. An indirect, belief-based, measure of attitude can be created by multiplying each behavioral belief by its corresponding outcome evaluation and then summing over outcomes. In a similar way, subjective norm is a function of the person’s beliefs that specific individuals or groups think he or she should, or should not, perform the behavior. A person who believes that most significant referents think he or she should perform the behavior will perceive social pressure to do so. Specifically, subjective norm is held to be a function of the person’s salient normative beliefs with respect to each referent, each weighted by their motivation to comply with that referent. An indirect measure of subjective norm can be created by multiplying each normative belief by its corresponding motivation to comply and then summing over referents.
Many behaviors cannot simply be performed at will; they require skills, opportunities, resources, or cooperation for their successful execution. The theory of planned behavior (TPB; Ajzen 1991) was an attempt to extend the TRA to include behaviors that are not entirely under volitional control, for example giving up smoking or using a condom. To accommodate such behaviors, Ajzen added a variable called perceived behavioral control to the TRA. This refers to the perceived ease or difficulty of performing the behavior, and is assumed to reflect past experience as well as anticipated obstacles. According to Ajzen, perceived behavioral control is a function of control beliefs in just the same way as subjective norm is a function of normative beliefs. It is assumed to have a direct influence on intention. For desirable behaviors, greater perceived behavioral control should lead to stronger intentions. Perceived behavioral control may also have a direct predictive effect on behavior, through two different mechanisms. First, holding intention constant, an individual with higher perceived behavioral control is likely to try harder and to persevere for longer than an individual who has lower perceived control. Second, people may have accurate perceptions of the amount of actual control they have over the behavior.
A number of meta-analyses of the TRA TPB have been conducted. The findings show that when intention is predicted from attitude and subjective norm, or from attitude, subjective norm and perceived behavioral control, between 40 and 50 percent of the variance is explained, on average. When behavior is predicted from intention alone or from intention and perceived behavioral control, between 19 and 38 percent of the variance is explained (Sutton 1998).
1.5 Comparison Of Social Cognition Models
The five social cognition models outlined above show a number of important similarities and differences. Some constructs are common to more than one model. For example, perceived susceptibility or perceived vulnerability occurs in both the HBM and PMT. Other constructs appear to be very similar, for example, perceived behavioral control and self-efficacy. Resolution of current controversies concerning the extent of overlap between such constructs requires the development of clear definitions, so that similar constructs can be distinguished on conceptual grounds, and more frequent tests of discriminant validity to investigate whether sets of apparently similar measures are tapping the same or different constructs.
All the models assume that individuals are future oriented and that they weigh up the costs and benefits of possible future courses of action. They all incorporate to a greater or lesser extent the expectancy–value principle which derives from the classical ex pected utility model, a normative model of decision making. In its weak form, this principle states that expectancies (subjective probabilities) and values are important determinants of behavior. In its strong form, the principle states that expectancies and values are combined multiplicatively, or at least that people behave as if they combine their cognitions in this way. Both the TRA and the TPB employ the strong form of the expectancy–value principle. The most systematic application of the principle is found in the subjective expected utility model (SEUM; Edwards 1954) which is based directly on expected utility theory. Versions of the SEUM have been applied to a number of health behaviors (e.g., Sutton et al. 1987). Researchers who use models such as the TPB and the SEUM need to be aware of the problems that arise from the use of multiplicative composites (Evans 1991).
This raises the thorny issue of rationality. Social cognition models are often criticized for offering an unrealistically rational account of how people form intentions and make decisions. However, the models do not imply that individuals always deliberate carefully and always make optimal decisions. People may not be aware of all the options available to them and of all the consequences that may follow from their actions. They may hold incorrect beliefs about the outcomes. They may make rapid decisions based on a few salient considerations. Having made a considered decision (e.g., to go jogging every Sunday morning), they do not necessarily have to weigh up the pros and cons again unless circumstances change; they may simply retrieve their previously formed intention from long-term memory and act on it. Thus, social cognition models imply a more limited rationality than is sometimes suggested by their critics.
Social cognition models are also sometimes criticized for being static. This criticism is unfounded: social cognition models summarize dynamic causal processes. In the TRA, for example, changes in behavioral beliefs and/or outcome evaluations are assumed to produce changes in attitude which in turn lead to changes in intention which ultimately produce changes in behavior. Models of health behavior should specify the time lags involved in these causal processes but most of them do not. However, it is often assumed implicitly that effects on intention are almost instantaneous whereas effects on behavior may be delayed.
Social cognition models differ in the degree to which they specify the content of the cognitions they identify. With the TRA, for example, once the behavior of interest has been defined, it is possible to generate questionnaire items for intention and for the direct measures of attitude and subjective norm. However, in order to generate items for behavioral beliefs, outcome evaluations, normative beliefs and motivations to comply, it is recommended that researchers gather information on salient beliefs from members of the target population. These constructs remain ‘contentfree’ until such information is obtained.
Compared with the other models, research on the TRA and the TPB shows a relatively high degree of standardization of measures based on published recommendations (Ajzen and Fishbein 1980). In addition, these authors emphasize the principle of correspondence (or compatibility) which, put simply, states that for maximum prediction the measures of all the constructs in the model should use similar wording. This principle is not widely applied in research using the other social cognition models.
The models also differ with regard to their scope of application. Key constructs in the HBM and PMT include perceived susceptibility and perceived severity with respect to a given health threat. Although these components can be extended to nonhealth-related events, for example the risk of financial loss, the scope of both models is necessarily limited by the nature of these two constructs. By contrast, the other three models are general theories that can be applied to any domain or behavior, for example voting, career, and purchasing decisions. Stated differently, SET, and the TRA and the TPB, regard health behaviors as having the same proximal determinants as other kinds of behavior. Thus, they offer the potential benefit of parsimony.
2. Stage Models
Stage models use similar concepts to social cognition models but organize them in a different way. They are fundamentally different in structure from social cognition models (Weinstein et al. 1998). According to this approach, behavior change involves movement through a sequence of discrete, qualitatively distinct, stages. Different factors are assumed to be important at different stages. Hence, people in different stages are assumed to require different interventions to encourage or help them to move to the next stage in the sequence.
Current models of health behavior that incorporate stage assumptions include: the transtheoretical model (TTM; Prochaska et al. 1992) and variants of it (e.g., De Vries and Mudde 1998), the precaution adoption process model (Weinstein and Sandman 1992), the health action process approach (Schwarzer and Fuchs 1996), and the health behavior goal model (Gebhardt 1997). This section focuses on the TTM because it is the dominant model in the field.
The TTM developed from studies of the processes of change in psychotherapy and smoking cessation. Smoking still accounts for the majority of applications of the model but it has been applied to a wide range of other health behaviors, including condom use, exercise, sunscreen use, and healthy eating (Prochaska and Velicer 1997). Although it is often referred to simply as the stages of change model, the TTM includes 15 different theoretical constructs drawn from different theories of behavior change. These include the stages of change (which provide the basic organizing principle), the 10 processes of change, the perceived pros and cons of changing, and self-efficacy and temptation. The TTM was an attempt to integrate these different constructs in a single comprehensive framework— hence the name transtheoretical.
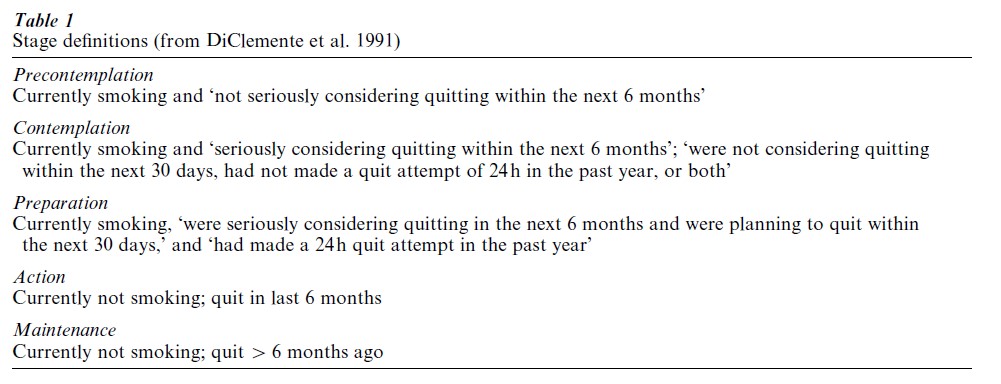
The version of the TTM used most widely in recent years specifies five stages: precontemplation, contemplation, preparation, action, and maintenance (DiClemente et al. 1991). Table 1 gives the operational definitions of the stages as applied to smoking cessation. Using a ‘staging algorithm,’ participants are classified into stages on the basis of their responses to a small number of questionnaire items. The first three categories contain the current smokers, the remaining two the ex-smokers; people who have never smoked are not represented in this scheme. Precontemplation, contemplation, and preparation are defined in terms of current intentions and past behavior (whether or not the person has made a 24 h quit attempt in the past year), whereas action and maintenance are defined purely in terms of behavior; ex-smokers’ intentions are not taken into account.
Prochaska et al. (1992) represented the stages of change as a spiral. People start at the bottom in precontemplation. They then move through the stages in order (contemplation, preparation, action, maintenance) but may relapse to an earlier stage. They may cycle and recycle through the stages several times before achieving successful long-term behavior change.
Of the other constructs in the TTM, the 10 processes of change refer to the things that people think and do to help them move through the stages, the pros and cons are the perceived advantages and disadvantages of changing, self-efficacy is borrowed from Bandura’s social cognitive theory, and temptation is a related concept that refers to the degree to which a person expects to feel tempted to lapse in different situations. The TTM is popular among clinicians and practitioners and there is a large body of evidence which is interpreted by its proponents as supporting the model. However, a closer examination of this literature reveals a number of serious problems with the TTM itself and with much of the research based on it (Sutton 2000). These problems include: lack of standardization of measures, particularly of the central construct of stages of change; logical flaws in current staging algorithms; inadequate specification of the causal relationships among the different constructs; misinterpretation of cross-sectional data on stages of change; and confusion concerning the nature of stage models and how they should be tested.
It is unfortunate that the model that has dominated the field to date is surrounded by a ‘thicket of problems,’ to use Bandura’s (1997) phrase. The notion that behavior change involves movement through a sequence of qualitative stages is an important idea that deserves further consideration. Health behavior researchers should turn their attention to the other stage models that have been proposed.
3. Conclusion
One focus of current interest is the ‘intention–behavior gap.’ Researchers in the health behavior field are using Gollwitzer’s (1993) concept of implementation intentions (the intention to do X in situation Y) and related ideas to explain why some people who have strong intentions to achieve a goal succeed whereas others fail, and to try to close this gap using simple interventions (e.g., Orbell et al. 1997). Related to this is the increasing interest in models of self-regulation (Abraham and Johnston 1998). Another trend, which has been apparent in social psychology in recent years and is now being imported into research on health behaviors, is to regard attitudes as being activated automatically (e.g., Fazio 1990). Although this seems to pose a challenge to social cognition models, the two approaches are not necessarily incompatible, especially if the idea is extended to automatic activation of previously formed intentions.
There is a plethora of models of health behavior and new models are continually being developed. Although this can be interpreted as a sign of a field rich in conceptual and theoretical development, it makes it increasingly difficult to accumulate research findings into a coherent body of knowledge. The field would benefit from clearer definition of concepts, greater standardization of measures, more tests of convergent and discriminant validity, greater concentration on a small number of models, and more empirical comparisons of models. The vast majority of studies use nonexperimental between-subjects designs. Obtaining repeated measures on the same individuals would allow models to be tested at the individual level (Hedeker et al. 1996). Experimental manipulation of constructs, as has been done in many studies of PMT, would provide much stronger evidence of causal effects.
Bibliography:
- Abraham C, Johnston M (eds.) 1998 Special issue on self-regulation and health. Psychology and Health 13: 565–766
- Ajzen I 1991 The theory of planned behavior. Organizational Behavior and Human Decision Processes 50: 179–211
- Ajzen I, Fishbein M 1980 Understanding Attitudes and Predicting Social Behavior. Prentice-Hall, Englewood Cliffs, NJ
- Bandura A 1986 Social Foundations of Thought and Action: A Social Cognitive Theory. Prentice-Hall, Englewood Cliffs, NJ
- Bandura A 1997 Self-efficacy: The Exercise of Control. Freeman, New York
- Becker M H (ed.) 1974 The Health Belief Model and Personal Health Behavior. Slack, Thorofare, NJ
- De Vries H, Mudde A N 1998 Predicting stage transitions for smoking cessation applying the attitude–social influence–-efficacy model. Psychology and Health 13: 369–85
- DiClemente C C, Prochaska J O, Fairhurst S K, Velicer W F, Velasquez M M, Rossi J S 1991 The process of smoking cessation: an analysis of precontemplation, contemplation, and preparation stages of change. Journal of Consulting and Clinical Psychology 59: 295–304
- Edwards W 1954 The theory of decision making. Psychological Bulletin 54: 380–417
- Evans M G 1991 The problem of analyzing multiplicative composites. American Psychologist 46: 6–15
- Fazio R H 1990 Multiple processes by which attitudes guide behavior: the MODE model as an integrative framework. Advances in Experimental Social Psychology 23: 75–109
- Floyd D L, Prentice-Dunn S, Rogers R W 2000 A meta-analysis of research on protection motivation theory. Journal of Applied Social Psychology 30: 407–29
- Gebhardt W A 1997 Health Behaviour Goal Model: Towards a Theoretical Framework for Health Behavior Change. University of Leiden, Leiden, The Netherlands
- Gollwitzer P M 1993 Goal achievement: the role of intentions. European Review of Social Psychology 4: 141–85
- Harrison J A, Mullen P D, Green L W 1992 A meta-analysis of studies of the Health Belief Model with adults. Health Education Research 7: 107–16
- Hedeker D, Flay B R, Petraitis J 1996 Estimating individual influences of behavioral intentions: an application of random-effects modeling to the theory of reasoned action. Journal of Consulting and Clinical Psychology 64: 109–20
- Janz N K, Becker M H 1984 The health belief model: a decade later. Health Education Quarterly 11: 1–47
- Milne S, Sheeran P, Orbell S 2000 Prediction and intervention in health-related behavior: a meta-analytic review of protection motivation theory. Journal of Applied Social Psychology 30 106–43
- Orbell S, Hodgkins S, Sheeran P 1997 Implementation intentions and the theory of planned behavior. Personality and Social Psychology Bulletin 23: 945–54
- Prochaska J O, DiClemente C C, Norcross J C 1992 In search of how people change: applications to addictive behaviors. American Psychologist 47: 1102–14
- Prochaska J O, Velicer W F 1997 The transtheoretical model of health behavior change. American Journal of Health Promotion 12: 38–48
- Rogers R W 1983 Cognitive and physiological processes in fear appeals and attitude change: a revised theory of protection motivation. In: Cacioppo J T, Petty R E, Shapiro D (eds.) Social Psychophysiology: A Sourcebook. Guilford Press, New York, pp. 153–76
- Schwarzer R, Fuchs R 1996 Self-efficacy and health behaviours. In: Conner M, Norman P (eds.) Predicting Health Behaviour: Research and Practice with Social Cognition Models. Open University Press, Buckingham, UK, pp. 163–96
- Sutton S 1998 Predicting and explaining intentions and behavior: how well are we doing? Journal of Applied Social Psychology 28: 1317–38
- Sutton S, Marsh A, Matheson J 1987 Explaining smokers’ decisions to stop: test of an expectancy-value approach. Social Behaviour 2: 35–49
- Sutton S A 2000 A critical review of the transtheoretical model applied to smoking cessation. In: Norman P, Abraham C, Conner M (eds.) Understanding and Changing Health Behaviour: From Health Beliefs to Self-Regulation. Harwood Academic Publishers, Amsterdam, pp. 207–25
- Weinstein N D, Rothman A J, Sutton S R 1998 Stage theories of health behavior: conceptual and methodological issues. Health Psychology 17: 290–99
- Weinstein N D, Sandman P M 1992 A model of the precaution adoption process: evidence from home radon testing. Health Psychology 11: 170–80
- Wurtele S K, Maddux J E 1987 Relative contributions of protection motivation theory components in predicting exercise intentions and behavior. Health Psychology 6: 453–66
ORDER HIGH QUALITY CUSTOM PAPER

Always on-time

Plagiarism-Free

100% Confidentiality