This sample health research paper features: 5800 words (approx. 19 pages), an outline, and a bibliography with 22 sources. Browse other research paper examples for more inspiration. If you need a thorough research paper written according to all the academic standards, you can always turn to our experienced writers for help. This is how your paper can get an A! Feel free to contact our writing service for professional assistance. We offer high-quality assignments for reasonable rates.
Abstract
Concepts of disease and health are often prompted by difficult cases. Does a person with a brain lesion that leads to desirable rather than undesirable behavior have a disease? How can we distinguish between health-affecting actions like hunger striking that are politically motivated and health-affecting actions like anorexia that may stem from diseased internal processes? The present research paper reviews concepts of health and disease that help address these questions. After outlining why bioethicists first started to debate concepts of disease, the different purposes that concepts of disease can serve are clarified: first is the mere conceptual correctness regardless of how the concept is used in medical practice; second is to guide interactions between those suffering from a condition and professionals like physicians or caregivers like friends and family members; third is to guide institutional decisions such as insurance reimbursement or disease manual revisions. The three major positions on how to conceptualize disease are discussed: naturalism, normativism, and hybrid theories. The virtues of each approach are outlined as well as problems each faces. Finally, the paper discusses how technological developments such as genetic testing and neuroimaging, which allow professionals to detect increasingly small changes in a person’s internal mechanisms, may affect concepts of disease and health.
Academic Writing, Editing, Proofreading, And Problem Solving Services
Gourmand: a man has a brain lesion. Before the lesion, he was fairly undiscriminating about the food that he ate, eating what his wife would prepare and only occasionally eating at restaurants; after the lesion, he became intensely focused on fine dining, seeking out the highest quality restaurants and switching his job to become a food columnist. Doctors trace the new behavior to a hemorrhagic infarction that has created a brain lesion near the man’s basal ganglia (Regard and Landis 1997).
Hunger striker: a person considers his imprisonment unjust and goes on a hunger strike to attract attention to his cause – he stops eating to protest his treatment at the hands of a governmental authority. Inspections by doctors reveal no abnormal brain activity associated with the strike.
Anorexic: a woman, unhappy with her body, decides to dramatically reduce the amount that she eats even though she knows that it may result in her death by starvation; she is diagnosed with anorexia nervosa, but doctors can find no abnormal brain activity associated with her decision to stop eating.
In which of these cases is the person suffering from a disease? To answer this question, we need to understand what makes a set of behaviors or a set of biological functions count as a disease or disorder, terms that the present research paper uses interchangeably. Does a large deviation from a statistically normal pattern of eating behavior make a person’s actions a disease – in which case hunger striker and anorexic certainly have a disease and gourmand might depending on the extent of his preoccupation? Does the fact that gourmand’s deviation is not considered harmful, while anorexic’s deviation is considered harmful matter for whether we consider each a disease? Does a disease need to be localizable to some clearly defined region of the body, in which case gourmand would suffer from a disease but not hunger striker or anorexic? These cases, and the questions that arise when trying to parse apart which count as a disease and which do not, illustrate the difficulty of outlining concepts of health and disease. Yet the cases also illustrate the importance of clarifying these concepts, for the cases highlight how our responses to each of these persons are shaped by our views about whether the person has a disease – does gourmand’s brain lesion need to be fixed? Should a physician force treatment (food) upon hunger striker?
In addressing these questions, the paper proceeds as follows and focuses on concepts of disease, which we can think of as picking out the range of ways in which a person can be unhealthy. First, the chapter outlines the background of debates over concepts of disease and health. Why did commentators become concerned with defining these terms? Second, why does defining concepts of disease matter – is conceptual truth the only goal of defining these concepts? Arguing against this view of the stakes of defining concepts of disease, the paper outlines implications that concepts of disease have for areas within bioethics like the physician-patient relationship and treatment priority setting. Third, the paper turns from defending why this debate matters to outlining the main positions on concepts of disease: naturalism, normativism, and hybrid theories of disease. Virtues of each approach, problems that each faces, and implications of each view of disease for debates in bioethics are reviewed. Finally, the paper touches on emerging discussions about concepts of disease that move beyond the longtime focus on debating naturalist versus normativist theories. These discussions underscore the need for closer interdisciplinary dialogue between philosophers concerned with what society ought to count as a disease and social scientists concerned with what society does count as a disease.
History And Development
When did commentators within philosophy of science, bioethics, and related disciplines first become concerned with defining concepts of disease and health? As Boorse (1977) and others point out, questions of what counts as a disease have often singled out one subset of disease entities – psychiatric categories – and questioned whether existing psychiatric categories captured “real” health problems or were formulated to control those who deviated from mainstream values within a society (Foucault 2001). The impetus to outline concepts of disease came from those skeptical that instead of treating disease, psychiatry was creating “an evaluator label that justifies the use of medical power.. .to intervene in socially disapproved behavior” (Wakefield 1992, p. 374).
These early foundations for trying to understand concepts of disease led to two research literatures with somewhat divergent trajectories. One literature focused on articulating a correct concept of mental illness and illustrating how psychiatry had failed to adhere to that concept when they labeled states like sadness or premenstrual problems as diseases (e.g., Caplan and Cosgrove 2004; Horwitz and Wakefield 2007). Another literature distanced itself from this project in two ways. First was a focus on both physical and mental illnesses. Second was an emphasis more on finding a correct concept of disease and less on identifying the ways in which existing medical practice deviated from that concept. For instance, although Boorse (1977) recognized that critiques of psychiatry provided a “strong motivation for trying to sort out various notions of health,” he and others hoped to move away from these critical accounts. This research paper , since it is focused on concepts of disease and health in general rather than concepts of psychiatric disease, will take up this latter stream of research. But it is important to recognize that the literature’s origins lied not only in getting the concept correct for correctness’ sake but in helping formulate concepts that would shed light on how social actors – psychiatrists, physicians, hospitals – should proceed in their treatment of various groups of persons.
Conceptual Clarification/Definition
The origin of debates over concepts of health illustrates that commentators often care about concepts of health for reasons beyond conceptual correctness or clarification. Indeed, commentators argue that concepts of health have important implications for concrete decisions by professionals, policymakers, and patients. Returning to the gourmand, hunger striker, and anorexia cases, we not only care about correctly classifying which of the persons have a disease but also care about clarifying the decisions that follow from that conceptual labeling. For instance, should an insurance company pay for corrective surgery for the gourmand? Therefore, before outlining the major positions on concepts of disease, the paper briefly outlines the different purposes commentators have for clarifying the concepts, drawing on Conrad’s (1992) discussion of the three levels at which a problem can be classified as a disease. Each level entails different debates for bioethics – for instance, how physicians should advise prospective parents about which diseases to test for prenatally versus how insurers should decide which treatments to reimburse.
First is the conceptual level, where a medical vocabulary is used to define a problem, even if medical professionals are not involved in treating the problem and medical solutions are not proposed. For instance, persons might begin to conceive of alcoholism as a medical problem involving dysfunctional reward circuits in the brain – yet the condition might still be predominantly treated by peers or other nonmedical professionals, and the treatments might be nonmedical in nature (e.g., a 12-step program) rather than medical (e.g., medication). Discussions of concepts of health and disease within the philosophy of science literature have often tried to restrict their scope to this level of defining disease. For instance, philosopher of science Schwartz, describing the positions of Wakefield and Boorse that are reviewed in the next section, argues that Wakefield and Boorse reject “any quick inference from disease-status of a condition to any conclusion about whether it should be treated or not.. .while both view medicine as having a particular interest in treating and preventing diseases, they agree it may be best to treat some non-diseases and not treat some diseases. Following them and others, the analysis will focus on the concepts of disease and dysfunction, avoiding conclusions about the advisability of medical interventions” (Schwartz 2007). At this level, the focus is on clarifying what should fall within the concept of disease rather than on how professionals and institutions should respond to diseases.
The second purpose for concepts of disease is to guide interactions between the person with the problem and physicians who frame the problem as medical for them and recommend medical interventions. So alcoholism may remain a disease at only the conceptual level if persons still seek help from 12-step programs and peers rather than medical professionals; when a person goes to a doctor who tells them that they have a disease and prescribes a medication, the concept guides an interaction rather than remaining a mere concept. This level for understanding concepts of health influences debates about how medical professionals should interact with those suffering from problems where the problem’s status as a disease is debated. For instance, the World Medical Association (WMA) forbids physicians from force-feeding hunger strikers but is careful to clarify that only some types of hunger striking are appropriately exempt from being treated as medical in physician interactions: “Individuals with seriously impaired mental capacity cannot be considered to be hunger strikers. They need to be given treatment for their mental health problems rather than allowed to fast in a manner that risks their health” (WMA Declaration of Malta on Hunger Strikers 2006). The WMA declaration is careful to distinguish when medical providers should treat a hunger striker as diseased in their interactions (if the person has seriously impaired mental capacities) versus when medical providers should not think of the hunger striker as diseased (if the person is competently deciding to strike). Disability-rights debates within bioethics also focus on whether it is appropriate for third parties interacting with the person with a disability to treat their differences as a disease. For instance, is it appropriate for a physician to offer cochlear implants for a child when the child’s parents view deafness as a cultural difference and may resent that interaction? Should a friend of a new parent whose child has a certain condition express sympathy for the disease or appreciate that child’s difference? Disease concepts thus shape how interactions between various agents – physician patient, teacher-student, and new parents and their friends – proceed.
The third and arguably most consequential purpose for disease concepts is to shape institutional decisions. Insurers must decide what counts as reimbursable diseases versus nonmedical problems. The committees behind disease classification systems must choose what belongs in a manual like the Diagnostic and Statistical Manual of Mental Disorders (DSM) or the International Classification of Disease (ICD) versus what should be excluded. Government research agencies must select which conditions should receive research funding. Courts may consider behavior linked to a disease as meriting more lenient punishment. Defining what counts as a disease may not be dispositive of these institutional decisions – that is, an insurance company may decide that something is a disease but that all the available treatments are too experimental to warrant medical insurance coverage. But the concept is nevertheless an important factor in these institutional decisions.
Ethical Dimensions
The first section outlined why a literature on concepts of health and disease has developed. It then clarified the different purposes that concepts of health and disease can serve. This section turns to the concepts themselves, outlining the three major positions on how to define disease – naturalism, normativism, and hybrid theories. It outlines merits of each approach as well as problems that each faces. For simplification purposes, the section focuses on an example theory in each category, which enables an analysis of broader between-group differences in each concept of health rather than more minor within-group disagreements.
Naturalism
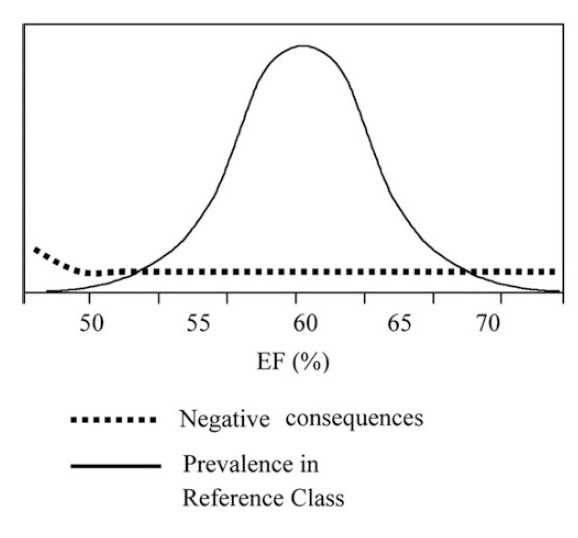
Naturalism (which is sometimes referred to as objectivism) seeks to define health and disease without relying on evaluative concepts about what makes a health state desirable or undesirable (Boorse 1977, 1997; Kendell 1975). Instead, Boorse (1977), who has proposed a biostatistical theory of disease, defines disease as follows. The first step in determining whether something is a disease is to choose a reference class for which it is appropriate to compare the functioning of members – for persons, it’s helpful to compare those of the same gender (to account for processes like childbirth) and of similar ages (to account for the fact that a 20-year-old’s parts likely function much better than an 80-year-old’s parts and that we would not want to label all 80-year-olds as diseased because of this difference). Second is to describe the parts of a person (e.g., her liver) as having a normal function, with normal defined as the statistically typical contribution by the organ or body part to the individual’s survival and reproduction. A disease is that which impairs a part’s normal functional ability (placing that part’s efficiency well below the statistical average of the part’s efficiency for other members of the reference group). Health is the absence of disease. Helpful for understanding Boorse’s theory is to imagine the diagram Boorse uses: a bell curve where the X axis represents degrees of an organ or part’s efficiency (e.g., a heart’s efficiency at pumping blood) and the Y axis represents the proportion of the reference group (e.g., 60-yearold males living in 2010) whose parts exhibit that degree of efficiency. Persons falling in the left-hand extreme of low efficiency have a part that is pathological. Persons falling in the rest of the curve have a non-pathological and thus healthy part. Framed in more concrete terms and drawing on Schwartz (2007), suppose that a statistically normal ejection fraction (EF), the amount of blood a heart pushes out per contraction, is 50%. Persons with EF’s around 50% have a non-pathological heart; those with an EF on the lower end of the distribution (20%) have a pathological and unhealthy heart (see Fig. 1 for Schwartz’s diagram).
The merits of naturalism are that it defines disease without reference to controversial assumptions about which health states are more versus less valuable. Instead of asking whether a person as a whole is healthy or unhealthy according to value-laden criteria, naturalism focuses not on an individual as a whole but on that individual’s component parts (organs, cells, bodily systems), examines the distribution of that part’s efficiency in contributing to that organism’s reproduction and survival, and then labels “unhealthy” any part that significantly deviates from the statistically average efficiency of contribution. In short, naturalism restricts its focus to analyzing (1) what functions of organs like a heart or lungs help an individual survive or reproduce, (2) what is the population-level distribution of that function, and (3) when does a part lie on the extreme end of that distribution. Boorse argues that these are biological questions rather than social or moral questions, thus creating a concept of disease useful for pathologists and others interested in identifying dysfunction. It also creates a concept of disease that can easily be applied to nonhuman animals and plants – entities that we speak of as diseased but that lack cultural values about what is harmful (Boorse 1977; Nordenfelt 2007).
Figure 1. Ranges of part efficiency (From Schwartz 2007, p. 378)
Yet Boorse’s theory, and similar ones in the vein of naturalism, encounters some problems. First and most fundamental is the problem of how to avoid normative concepts when evaluating whether an organ or bodily system is functional or dysfunctional. Boorse defines a part’s function by its contribution to an individual’s survival and reproduction. But as others note, there are many goals that an individual can pursue and to which an organ or bodily part can contribute. As Ereshefsky (2009) puts it, many of an individual’s states play no direct role in her survival or reproduction – “eating for eating’s sake.. .nonreproductive sex” (p. 223). The claim here is that the decision to focus on an organ’s contribution to two specific human goals – survival and reproduction – is a value-laden decision to prioritize some human goals over others.
Another fundamental criticism of Boorse and other naturalist theories is that they fail to reflect changes in the functioning of bodily parts that may be statistically deviant but that a person or a culture does not consider harmful. Homosexuality may reduce a person’s ability to reproduce by natural means and perhaps survive, but organizations like the American Psychiatric Association (APA) have removed it from their disease classification systems under the premise that it is not harmful. In the gourmand case outlined at the outset of this chapter, where a man’s brain lesion leads to a sudden urge for fine cuisine, some would hesitate to call the lesion a disease if neither the man nor those around him considered the lesion’s effects harmful or would seek to avoid the lesion’s effects.
Finally, though Boorse seeks to avoid drawing inferences from what conceptually is diseased to how medical practitioners and social institutions should treat those whom his concept identifies as diseased, adopting his theory could have implications for debates within bioethics such as priority setting for the allocation of healthcare resources for different medical conditions. These allocations often draw upon scales that measure how harmful a health condition is by asking how the condition impedes a range of goals a person has beyond survival and reproduction – for example, a person’s mobility or ability to dress himself each day. And focusing on this broader range of harms reveals cultural variability in the harm a condition causes – for instance, fine-grained eyesight issues may cause greater harm in literacy-heavy societies than in agricultural ones. Those who adopt a naturalist theory of disease that focuses on an organ’s contribution to survival and reproduction, rather than that organ’s contribution to a broader range of harms that may be culturally variable, may end up with different healthcare allocation priorities. For instance, lower back pain may impede daily tasks but have no effect on survival or reproduction, not meriting inclusion in allocation theories that draw solely on Boorse’s concept. This shows how although naturalist theories focus on conceptual correctness rather than ethical implications, how they define what counts as dysfunctional can still matter for applied debates within bioethics.
Normativism
While those working within naturalism see their theory’s avoidance of judgments about what health states should count as harmful as an attraction of their approach, those working within normativism (which can also be called constructivism) argue that concepts of disease do and perhaps should involve cultural judgments about what makes a life go badly. Returning to the gourmand case, Boorse’s theory of disease might claim that because the man has a bodily organ (a brain region) that makes a statistically deviant contribution to survival and reproduction, the man suffers from a disease; a normativist might point out that because the changes in the man – his newly discerning epicurean palate – are culturally valued, the man is perfectly healthy. As some have pointed out, normativists are often less interested in outlining a precise concept of health or disease and more interested in investigating the historical and social processes through which society comes to disvalue some states or behaviors, for example, fatness, and label the problem as medical (for a discussion of this focus of normativist theories, see Murphy 2009). Nevertheless, some theorists do provide rigorous, normativist concepts of health (Engelhardt 1996; Nordenfelt 1995). The focus here is on Nordenfelt (1995).
Recall that a main criticism of Boorse’s statistical theory of disease was that it prioritized a certain set of goals of an organism – survival and reproduction – while claiming that this prioritization did not stem from human values about the function that a person’s bodily systems should serve. In Nordenfelt’s theory, which he labels the holistic theory of health (HTH), he argues that survival and reproduction are only two among many goals to which a healthy organ or bodily system’s functioning should contribute. Instead of focusing solely on survival and reproduction and instead of focusing on specific organs or bodily systems, the HTH focuses on a broader array of goals – vital goals a person defines for herself that are necessary and sufficient for a minimal level of happiness – and asks whether the whole person has the ability to pursue all of his or her vital goals (in which case she is healthy) or whether suffering or disability impedes the person’s pursuit of those goals (in which case she is diseased or unhealthy). In other words, a person’s subjective values about goals he wishes to pursue will shape what is considered disease (Nordenfelt 1995).
Theories of disease within normativism appear to correctly point out why diseases matter morally – why governments have an obligation to alleviate disease among their citizens and why one expresses pity for a friend who relays the suffering that his/her disease causes. But normativist theories can fail to distinguish between the following: (1) states that are disvalued or that block vital goals and that should be considered diseases or medical problems versus (2) states that are disvalued or that block vital goals but that should be considered moral problems, social problems, etc. (Cooper 2002; Murphy 2009). While some social scientists have argued that society increasingly labels violations of moral norms such as murders or sexual aggression as “mad” (diseases) rather than “bad” (moral failings) (Szasz 2007), there are still behaviors that society disvalues but that few would argue should be labeled as medical problems. For instance, a day care worker murdering a child out of extreme annoyance at his crying is socially disvalued but still likely to be properly classified as criminal or immoral in most cases rather than diseased.
Likewise, disability and suffering may block a person’s vital goals but seem inappropriate to be considered a disease. For example, a woman may experience very low self-confidence due to extreme workplace sexism that blocks her vital goal of maintaining an active career. It seems clear that sexism-induced suffering or disability is not a medical problem but a different sort of problem requiring a very different set of institutional responses. Therefore, theories that define disease solely in reference to states that are culturally disvalued or states that impede a person’s valued goals can fail to distinguish between problems from disease and problems from other sources. This could have implications for bioethics. For example, debates about whether medical technologies like ADHD medication are the proper solution to attention-related suffering or whether the problem would be better alleviated by smaller class sizes, more recess, and other nondisease related solutions, focus on whether the source of the problem lies primarily in biology or in social arrangements. A theory that focuses more on the presence of harm rather than whether there is a biological source to the harm could deflect attention from problems with largely nonmedical origins best served by nonmedical solutions.
Hybrid
Normativist theories face the problem of distinguishing between states that society disvalues and that should count as a disease and states that society disvalues but that should not count as disease. Hybrid theories try to overcome this problem by investigating whether the harm or social disvalue that normativists focus on is traceable to dysfunctional bodily mechanisms rather than dysfunctional moral or social situations. Wakefield (1992), who sets forth one of the most prominent hybrid theories, does so by arguing that a condition is a disorder if it meets two necessary and sufficient criteria. First, and drawing upon normativist theories of disease, is whether a condition causes some harm or deprivation of benefit to the person as judged by the standards of a person’s culture (Wakefield 1992). Second is whether the condition results from an internal bodily mechanism not performing its natural function, with “natural” referring to the function that natural selection chose. Thus, a person who commits socially disvalued murder would not have a disease unless the murder was a result of an internal bodily mechanism not performing the function for which it was selected; conversely, the gourmand’s appetite for fine food, though it results from a lesion that represents an internal mechanism deviating from its selected-for function, would not count as a disease since the person’s behavior is not harmful according to the standards of his culture. The appeal of hybrid theories is that they ensure that we only count conditions as a disease if the condition causes harm but that we filter the set of harm-causing problems to ones that stem from bodily dysfunction rather than social dysfunction, prejudice, moral failings, or other sources.
What problems and drawbacks do hybrid theories face? First is that while normativism seems to label too many problems as disease, hybrid theories, by applying two requirements for what counts as a disease, may commit the opposite problem and label too few problems as a disease. Ereshefsky (2009) gives the example of a female unable to orgasm because of a problem with a part of her female organs. Because the female organs were not selected for by evolution for the purpose of female orgasm – instead, evolution selected for what would help produce male orgasms, with female orgasms as a byproduct – the problem would fail to satisfy Wakefield’s second criterion and thus fail to count as a disorder (or disease, in our terms). Yet Ereshefsky points out that because the problem satisfies the first criterion – it is harmful – and because it is traceable to a problem with a bodily organ, we might want to count the problem as a disease. Other hybrid theories try to correct for this problem by arguing that for a condition to count as a disease, it should be both harmful and potentially remediable by medical treatment (thus including the female orgasm problem as a disease, while excluding problems like sexism-induced workplace difficulties that are not potentially solvable by medical remedies) (Cooper 2002). This illustrates that while hybrid theorists seem to agree first on the harmful criterion and second that this criterion needs to be supplemented by some reference to the harm being caused by a bodily dysfunction or medically treatable condition, there remains work to be done in clarifying the “dysfunction” criterion in the definition.
While the first problem with hybrid theories stems from combining a harm criterion with a dysfunction criterion, the second problem that emerges is that even if one accepts that there should be a dysfunction requirement, it is not clear why an organ’s present function should be evaluated in terms of the function that natural selection chose for the organ. Some point out that natural selection merely favors what offers an organism a comparative advantage at the time rather than an advantage we would presently value; for instance, a condition that produces a heart that allows 1% of children to survive is selected over a condition that allows 0.1% of children to survive, but it is not clear that hearts should be assessed as diseased or not diseased according to this 1% standard of survival (Schwartz 2007). Others point to problems with identifying which stage of natural selection should be used to define a part’s function (Cooper 2002). For instance, fat storage capabilities that were once selected for in times of scarcer food supply are now selected against – which selection should define the storage capability’s functions? These questions, though not fatal to hybrid theories, point to the need for continued work on defining what counts as dysfunctional.
An Emerging Conceptual Health Issue
While much bioethical discussion concerning concepts of health and disease has focused on debates between the above positions, an emerging issue for concepts of disease and health stems from empirical developments in how society defines and treats disease. The development is medicine’s increasing focus on treating risk factors such as high blood pressure or cholesterol that increase a person’s risk for future suffering but that cause the person no suffering at present.
Technological developments have facilitated medicine’s focus on risk, from tests to detect elevated blood pressure or blood-borne levels of insulin (Greene 2008) to genetic tests that examine mutations such as BRCA that predict elevated risk of breast cancer to neuroimaging that aims to detect when neural development starts to go awry, putting persons at elevated risk for mental illnesses like schizophrenia or anxiety disorder. Do the small physiological deviations that put a person at risk for later suffering, which often compose risk syndromes, constitute a disease in and of themselves?
Addressing this question, existing concepts of health and disease seem divided along two lines. First is whether the concept argues that disease can occur if a small part of a person is malfunctioning or whether the concept argues that disease should be restricted to situations where the whole person is malfunctioning rather than a small part. Falling in the former category, for instance, is Boorse (1987), who argues that liver cells can be diseased if they are not performing their appropriate metabolic function even though the overall organ may not be malfunctioning at a level significantly below normal. Since risk syndromes often describe subtle dysfunctions in cells or organs – in the circulation of blood or how a particular brain region develops – theories such as Boorse’s that focus on dysfunction at the level of small parts of the organism rather than dysfunction at the level of the whole organism seem to capture risk syndromes as diseases. In contrast, theories such as Nordenfelt (1995) that argue that disease occurs when the whole person is blocked from realizing important goals are more likely to see small physiological deviations as putting a person at risk for future disease rather constituting diseases in and of themselves.
Another division occurs between theories that focus on objective accounts of the harm a person experiences from disease – does the disease impede what is in a person’s interest, such as survival? – versus theories that focus on subjective accounts of the harm a person experiences from disease – does a disease cause a person to feel suffering or frustration at a blocked pursuit of goals? Since risk syndromes rarely cause a person to feel worse or feel that they are suffering, concepts of health and disease that draw upon the latter form of harm will be less likely to count these syndromes as present diseases. These questions have been present throughout the conceptual clarification of health and disease, but developments that allow medicine to detect increasingly minute physiological changes increase their importance.
Conclusion
The present research paper focused on concepts of health and disease. First, it reviewed the development of efforts at clarifying these concepts, illustrating how an initial singling out of psychiatry and its disease categories soon expanded to a focus on a broader range of ailments. After reviewing the debate’s history, it outlined the different stakes of defining concepts of disease, drawing a distinction between goals of conceptual correctness, goals of guiding between-person interactions, and goals of guiding institutional decision-making. Having illustrated these stakes, three major positions on how to define health and disease were described – naturalism, normativism, and hybrid theories – with benefits and drawbacks of each highlighted. Concluding, it is important to note a couple topics omitted given the scope of the present review. First are debates over whether persons should only use medical technologies to help them function closer to the average person or whether they can use “enhancing” technologies to help them function at levels above the average person. These debates draw on concepts of disease that distinguish between normal and subnormal levels of functioning. Second are debates over whether persons have a “right” to health that governments are obligated to satisfy if they have appropriate resources: Is there a right to health? Is it best satisfied by the provision of medical technologies or by improvements in social factors like housing and sanitation? Do persons have a right to assistance achieving some minimal level of health? These questions draw upon concepts of disease and health. For now, the present chapter highlighted important positions on fundamental concepts of disease and health that can help inform these other debates within global bioethics.
Bibliography :
Boorse, C. (1977). Health as a theoretical concept. Philosophy of Science, 44(4), 542–573.
Boorse, C. (1987). Concepts of Health. In D. Van De Veer and T. Regan (Eds.), Health Care Ethics: An Introduction (pp. 359–393). Philadelphia: Temple University Press.
Boorse, C. (1997). A rebuttal on health. In J. M. Humber & R. F. Almeder (Eds.), What is disease? (pp. 1–134). Totowa: Humana Press.
Caplan, P. J., & Cosgrove, L. (2004). Bias in psychiatric diagnosis. Lanham: Rowman & Littlefield.
Conrad, P. (1992). Medicalization and social control. Annual Review of Sociology, 18, 209–232.
Cooper, R. (2002). Disease. Studies in History and Philosophy of Science Part C: Studies in History and Philosophy of Biological and Biomedical Sciences, 33(2), 263–282.
Engelhardt, H. T. (1996). The foundations of bioethics (2nd ed.). New York: Oxford University Press.
Ereshefsky, M. (2009). Defining ‘health’ and disease. Studies in History and Philosophy of Science Part C: Studies in History and Philosophy of Biological and Biomedical Sciences, 40(3), 221–227.
Foucault, M. (2001). Madness and civilization: A history of insanity in the age of reason. New York: Psychology Press.
Greene, J. (2008). Prescribing by numbers: Drugs and the definition of disease (1st ed.). Baltimore: Johns Hopkins University Press.
Horwitz, A. V., & Wakefield, J. C. (2007). The loss of sadness: How psychiatry transformed normal sorrow into depressive disorder (Vol. xv). New York: Oxford University Press.
Kendell, R. E. (1975). The concept of disease and its implications for psychiatry. The British Journal of Psychiatry, 127(4), 305–315.
Nordenfelt, L. (1995). On the nature of health: An actiontheoretic approach. Dordrecht: Springer.
Nordenfelt, L. (2007). The concepts of health and illness revisited. Medicine, Health Care and Philosophy, 10(1), 5–10.
Regard, M., & Landis, T. (1997). “Gourmand syndrome” eating passion associated with right anterior lesions. Neurology, 48(5), 1185–1190.
Schwartz, P. H. (2007). Defining dysfunction: Natural selection, design, and drawing a line. Philosophy of Science, 74(3), 364–385.
Szasz, T. (2007). The medicalization of everyday life: Selected essays. Syracuse: Syracuse University Press.
Wakefield, J. C. (1992). The concept of mental disorder: On the boundary between biological facts and social values. American Psychologist, 47(3), 373–388.
Reznek, L. (1987). The nature of disease. London: Routledge & Kegan Paul.
Sisti, D. (2009). Health and disease: Conceptual perspectives and ethical implications. In V. Ravitsky, A. Fiester, & A. Caplan (Eds.), The Penn Center guide to bioethics. New York: Springer.