
View sample cancer research paper on cancer epidemiology. Browse other research paper examples for more inspiration. If you need a thorough research paper written according to all the academic standards, you can always turn to our experienced writers for help. This is how your paper can get an A! Feel free to contact our writing service for professional assistance. We offer high-quality assignments for reasonable rates.
Cancer Distribution Worldwide
Cancer is a major public health problem throughout the world, causing more than a quarter of all deaths in many countries. Cancer accounted for approximately 7 million deaths worldwide in 2002, one in eight of all deaths. In the same year, 11 million people were diagnosed with cancer and nearly 25 million people diagnosed with cancer over the previous 3 years were still alive (Parkin et al., 2005). The absolute number of people diagnosed with cancer is increasing steadily because of continuing increases in life expectancy and world population, and it has been estimated that there will be 15 million new cases per year by 2020.
Academic Writing, Editing, Proofreading, And Problem Solving Services
Get 10% OFF with 24START discount code
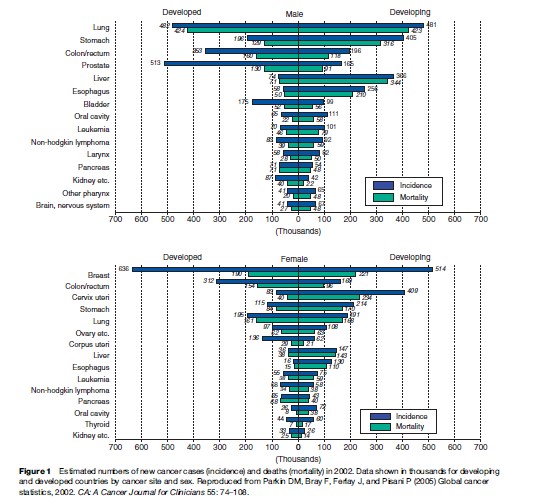
Lung (1.4 million cases), breast (1.2 million cases), and colorectal (1 million cases) cancer are the most commonly diagnosed cancers, whereas lung cancer (1.2 million cancer deaths), stomach cancer (700 000 deaths), and liver cancer (600 000 deaths) are the most common causes of cancer death (Parkin et al., 2005).
Numbers of new cancer cases (incidence) and deaths (mortality) in 2002 are presented in Figure 1 for developed and developing countries. The ratio of mortality to incidence reflects the fatality rate of the cancer. Pancreas and liver cancer, for instance, have similar incidence and mortality because their prognosis is poor. Breast cancer has a relatively good prognosis, so mortality is much lower than incidence, particularly in developed countries.
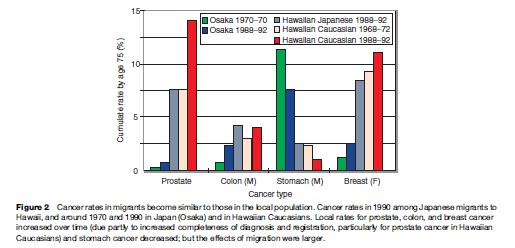
Many types of cancer vary in incidence by more than one order of magnitude between different populations, and every type is rare in some part of the world (Doll and Peto, 1981). The convergence toward local cancer rates seen among immigrants (Figure 2) excludes a genetic explanation of these differences. By the 1960s, cancer epidemiologists had therefore concluded that most cancers are in principle preventable and many could be avoided by a suitable choice of lifestyle and environment. Many specific causes of cancer are now known, the most important being smoking, obesity, and a few cancer-causing (oncogenic) viruses, but a large proportion of global variation for common cancers such as breast, prostate, colon, and rectum remains unexplained.
Age-specific cancer incidence and mortality rates have fallen for some cancer sites, while other cancers have become more common, reflecting changes in relevant exposures, diagnosis, treatment, and screening. Increases in cigarette smoking since the 1950s caused large increases in death rates for smoking-related cancers, but overall mortality from cancers not caused by smoking has generally decreased or remained stable in most Western countries (Peto et al., 2006).
Effect Of Cancer Screening On Incidence And Mortality
Cancer screening programs can reduce mortality by early detection of the disease and hence earlier treatment, but for some cancers the benefit may be too small to justify the costs. Well-organized cervical screening prevents the majority of cervical cancers by detecting and treating premalignant disease, but for breast and prostate cancers mortality is reduced while cancer incidence is increased by screening, because early cancers are detected that would never have become symptomatic. Widespread prostate specific antigen (PSA) testing from around 1986 onward has caused an enormous increase in the incidence of prostate cancer in the United States, followed a few years later by smaller increases in other countries, but has had only a small effect on mortality.
Population screening for colorectal cancer has recently been introduced in some Western countries, but its long-term impact on mortality and morbidity in a population setting will not be known for many years. Studies on the benefits of lung cancer screening are ongoing. Some screening programs are targeted at individuals at high risk, particularly people with a strong family history of the disease.
Environmental And Lifestyle Causes Of Cancer
Carcinogenic Effects Of Tobacco
The most important discovery in the history of cancer epidemiology is the carcinogenic (cancer-causing) effect of tobacco. Lung cancer incidence increases rapidly among continuing smokers, but remains roughly constant in ex-smokers. The risk is therefore greatest in those who begin to smoke when young and continue throughout life. Secondhand, or environmental, tobacco smoking is also carcinogenic, but it is hard to quantify the magnitude of the risk.
The large increase in male cigarette smoking in most developed countries that occurred during the first half of the twentieth century caused an unprecedented epidemic in the lung cancer rate several decades later. A reduction in tar levels in cigarettes combined with decreases in smoking has subsequently reduced the lung cancer rate in many developed countries. Women in most Western countries began smoking later than men and fewer have stopped, so their lung cancer rates are either still increasing or falling less rapidly.
For many years, the carcinogenic effects of tobacco were thought to be restricted largely to the lung, pancreas, bladder, and kidney, and (synergistically with alcohol) the larynx, mouth, pharynx (except nasopharynx), and esophagus. More recent evidence indicates that stomach, liver, cervix, myeloid leukemia, and probably colorectal cancer are also increased by smoking. This makes smoking the most important known risk factor for cancer.
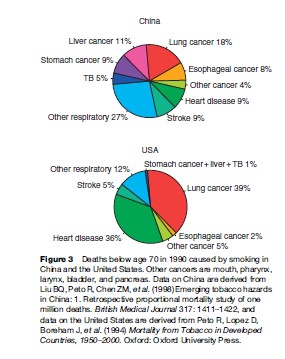
The relative importance of different smoking-related diseases varies widely between populations, as smoking usually multiplies the background rate due to other factors. In China, where liver cancer is common, smoking causes more premature deaths from liver cancer than from heart disease, while in the United States liver cancer is rare even in smokers (Figure 3).
The Effects Of Diet And Overweight
Nutritional epidemiology is notoriously complex owing to the variety of foods and their many constituents and to intercorrelations and temporal changes in their patterns of use. Cancer risks in old age may also depend as much on diet in early life as on current habits.
Most dietary factors do not show a strong and consistent enough effect to establish them unequivocally as important carcinogens or anticarcinogens. Exceptions are drinking alcohol, consumption of various foods contaminated with aflatoxin, and a few local customs (such as feeding Chinese-style salted fish to infants, which causes nasopharyngeal cancer). Extensive research during the past two decades has shown that rates for various cancers correlate fairly consistently with certain aspects of diet, but opinions still differ on the strength of the evidence. In the 1980s, nutritional epidemiology focused mainly on meat, fat, and total energy intake as potential risk factors, and on dietary fiber, fruits, and vegetables, vitamins A, C, and E, and b-carotene as protective factors. More recent research has concentrated on red and processed meat as risk factors, and on folate and other B vitamins, vitamin D and calcium, selenium and specific non-nutrient components of fruits, vegetables, and whole grains (e.g., phytoestrogens and isothiocyanates present in cruciferous vegetables) as protective factors. The overall evidence that fats are hazardous and fruits and vegetables are protective seems less convincing than initially thought, and more specific compounds and mechanisms are being investigated. Fat is classified according to its source (animal or vegetable fat) and its different subtypes (e.g., saturated fat). A high intake of n-3 fatty acids, derived from fatty fish, may prove to be beneficial. The evidence on diet and cancer has been systematically reviewed and summarized by the World Cancer Research Fund/American Institute for Cancer Research in 2007.
Dietary supplements may not have the same effects as the foods that contain them, and some may even be harmful. For example, b-carotene appeared to be associated with reduced risk of cancer in observational studies, but 12 years of treatment in a large randomized trial showed no benefit, and in two shorter trials the lung cancer risk was higher in those who received b-carotene supplements (Greenwald et al., 2007). Aspirin probably reduces colorectal cancer incidence but may take a decade or more to do so.
Most reports conclude that about one-third of cancer deaths might be avoidable by dietary change. However, dietary recommendations differ, and Doll and Peto (2005) concluded that only cancers due to obesity are definitely avoidable. Radical changes in national dietary habits would not be easy to achieve even if there were a consensus on which foods are relevant.
There is now a consensus that cancer is commoner in those who are overweight. The evidence on weight is strongest for postmenopausal breast cancer and cancers of the endometrium, gallbladder, and kidney, but several other sites contribute to the observed overall cancer risk. A large prospective cohort of nonsmokers in America, where obesity is particularly common, provides the strongest evidence on the association between body mass index (BMI; weight divided by the square of height) and cancer mortality (Calle et al., 1999). The authors did not calculate an attributable fraction, but if the observed excess mortality reflects a direct effect their data suggest that approximately 10% of all cancer deaths among American nonsmokers (7% in men and 12% in women) would be avoided if no one’s BMI exceeded 25 kg/m2. It is, however, not clear how much the risk can be reduced by weight reduction in those who are already overweight. Mortality from nonmalignant diseases is increased in those who are either too thin or too fat. Since obesity is an increasing problem in Western societies, the number of weight-related cancers will inevitably increase in the years to come.
Reproductive And Hormonal Factors
The effects of reproductive factors on breast and ovarian cancer have long been assumed to reflect underlying hormonal processes, and this is confirmed by the effects of both endogenous and exogenous hormones. Breast cancer incidence is transiently increased by pregnancy and while estrogens are administered as oral contraceptives or hormone replacement therapy (HRT), and is permanently lowered by late menarche, early menopause, early first childbirth, and high parity. Endometrial cancer incidence is also transiently increased by HRT. Combined estrogen and progestin HRT has a larger effect than estrogen alone for breast cancer, but a smaller effect for endometrial cancer. Ovarian cancer incidence declines with increasing parity, and both endometrial and ovarian cancers are less common in oral contraceptive users. Both oral contraceptives and HRT appear to reduce colorectal cancer incidence.
The Western diet is associated both with earlier age at menarche and with postmenopausal obesity, which increases endogenous estrogen production. Breast cancer incidence is much higher in most Western countries than in many developing countries, and this is partly (and perhaps largely) accounted for by these dietary effects combined with later first childbirth, lower parity and shorter breastfeeding. The development of cancers of the testis and prostate may also depend on hormonal effects, but apart from the increased risk in an undescended testis, no behavioral or reproductive correlate is strongly predictive of these diseases.
Viruses, Bacteria, And Parasites
Important discoveries of the past 30 years in cancer epidemiology relate to the carcinogenic effects of infectious agents. Recent estimates of the global cancer burden caused by specific viruses, bacteria, and parasites (Parkin, 2006) imply that about 20% of all cancers worldwide are caused by known infections (Table 1).
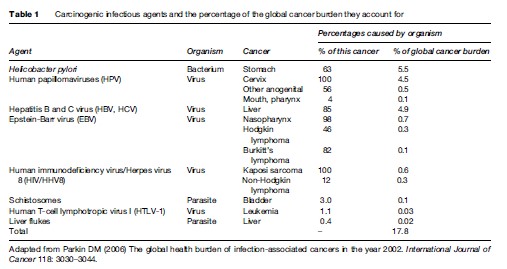
Helicobacter pylori, a chronic gastric bacterial infection that can cause gastric ulcers, is a major factor in the development of stomach cancer, accounting for an estimated 63% of all stomach cancers and 5.5% of all cancers worldwide. The evidence is particularly strong for noncardiac gastric cancers, which comprise more than 80% of gastric cancers. H. pylori is common in developed and developing countries, and more than half of all stomach cancers might be prevented if H. pylori could be eradicated.
More than 100 human papillomaviruses (HPVs) have been identified, and DNA from a subgroup of sexually transmitted HPVs that includes HPV16, HPV18, and HPV45 is detectable in virtually all cervical cancers worldwide. These and other HPVs are also found in other anogenital cancers, and in some cancers of the mouth and pharynx. HPV vaccines are now available, but their longterm effect on overall cervical cancer incidence remains to be established. At present, the high cost of HPV vaccines precludes their widespread use in developing countries that lack the resources for organized cervical screening, where their potential impact is greatest. Their effect in countries that already have effective screening is unclear. They are only effective against specific HPV types, so they will not prevent all cervical cancers; they are unlikely to be effective in women who have already been infected; and vaccinated women may be less likely to participate in cervical screening, which is known to be very effective.
The contribution of hepatitis B virus (HBV) to liver cancer in high-incidence regions has long been recognized, and the hepatitis C virus (HCV) is similarly carcinogenic. Hepatitis B infection is common in developing countries, and together with hepatitis C it accounts for 85% of all liver cancers worldwide (Parkin, 2006). The incidence of several virally induced cancers is further increased by specific cofactors such as salted fish (nasopharynx), smoking (liver and cervix), aflatoxin (liver), and malaria (the major cofactor with EBV for Burkitt’s lymphoma in Africa). There is also strong epidemiological evidence for an infective etiology in childhood leukemia, but no specific pathogen has been implicated. Therapeutic immunosuppression causes a marked increase in the incidence of non-melanoma skin cancer and some virally induced cancers. The discovery that many other epithelial cancers are also increased by immunosuppression (Buell et al., 2005) suggests that unidentified viruses may be important in these cancers as well. The alternative is the long-standing but equally speculative theory that many nonviral cancers are normally kept in check by the immune system.
Occupational And Environmental Carcinogens
Roughly a dozen specific occupational exposures and several complex mixtures, particularly the combustion products of coal, have caused high risks of certain cancers (predominantly lung cancer) in heavily exposed workers. Exposure levels for many industrial hazards have been progressively reduced in many Western countries since the 1930s, and by the late 1970s it was assumed, probably correctly, that the occupational exposure levels then current would contribute a very small proportion of future cancer incidence. But uncontrolled asbestos use had been widespread in the construction industry in Western countries from the 1950s to the mid-1970s, when public concern led to a rapid reduction. The resulting epidemic of mesothelioma in building and other workers born after 1940 did not become apparent until the 1990s because of the long latency of the disease. Incidence rates are still rising, and asbestos exposure prior to 1980 may eventually cause 250 000 mesotheliomas and a similar number of lung cancers in Western Europe. Chrysotile (white asbestos) causes a much lower mesothelioma risk than other types, but all forms of asbestos cause cancer.
This tragic episode was largely avoidable, as the carcinogenic effects of asbestos were known by 1960; but it illustrates the major weakness of epidemiology as an early warning system. The increase in cancer incidence caused by increased exposure to a carcinogen might not be detectable for several decades, and laboratory testing must remain the first line of defense against potentially dangerous new agents, particularly those affecting endocrine or paracrine signaling that could be biologically active at very low levels.
Epidemiological studies of markers such as DNA adducts in the lung or chromosomal aberrations in lymphocytes might also provide early warning of a potential hazard. But such direct or indirect measures of mutagenic or transforming potency have never detected an important carcinogen and even today cannot provide quantitative estimates of risk.
Epidemiological data on human cancer rates still provide the only reliable evidence that the cancer risks caused by long-established activities such as working in an oil refinery or living near a high-voltage power line are not large. There is as yet little evidence of a link between mobile phone use and cancer risk, but it may be too early for an effect to be detected. Apart from melanoma and other (usually nonfatal) skin cancers due to excessive exposure to sunlight, the only substantial and widespread cancer risk known to be caused by an avoidable environmental factor in developed countries is the further increase in lung cancer among smokers caused by indoor radon escaping from the ground or from building materials, although both indoor and outdoor air pollution from fossil fuels may also contribute to the risk in smokers. The risk to nonsmokers is relatively trivial in developed countries, but burning fossil fuels indoors without adequate ventilation certainly contributes to the high lung cancer rates, even in nonsmokers, seen in parts of China.
Genetic And Molecular Epidemiology Of Cancer
An inherited mutation that predisposes carriers to cancer often involves a gene that is mutated or deleted during the transformation of a normal cell to cancer in people who have not inherited a defective gene. Some of these genes affect metabolism of carcinogens, but many are involved in normal cellular mechanisms such as detection and repair of DNA damage, control of the cell cycle, or apoptosis (programmed cell death). They have been discovered in many ways, notably by laboratory studies of such pathways, linkage in families with cancer syndromes such as hereditary retinoblastoma, DNA sequence homology with oncogenic viruses, and recently by direct comparison of normal and tumor DNA, which is now being done systematically throughout the genome for a few cancers.
Polymorphisms In Candidate Genes
There have been many studies comparing the prevalence in cancer patients and unaffected controls of differences in DNA sequence in genes involved in the metabolism of external or endogenous mutagens or in the production or processing of sex hormones or their analogs. A few polymorphisms in such genes seem to alter the risk substantially, such as the N-acetyltransferase 2 (NAT2) variant underlying the slow acetylator phenotype, which increases the risk of bladder cancer, particularly in workers heavily exposed to certain aromatic amines. But systematic metaanalysis reveals little or no effect for most such single polymorphisms, and the pooled data for the minority that are statistically significant usually suggest carrier:noncarrier risk ratios of less than two, and often much less.
There have been various reports of statistically significant gene–environment interactions, such as a much larger lung cancer risk due to passive smoking in women with glutathione S-transferase m1 (GSTM1) deficiency, or an increased breast cancer risk due to smoking in postmenopausal women that was confined to NAT2 slow acetylators. In these examples, however, the estimates of the risk in susceptibles (although not their lower confidence limits) were inconsistent with the much lower overall effect of passive smoking on lung cancer or of smoking on breast cancer (which is nil) in larger studies. Many apparently significant gene–gene or gene–exposure interactions will arise by chance, but some will be real. The reported interaction between a polymorphism in the methylenetetrahydrofolate reductase (MTHFR) gene and dietary folate in colorectal cancer is a biologically plausible mechanism with epidemiological support.
Familial Risks For Common Cancers
Hereditary cancer syndromes caused by an inactivating mutation in a single crucial gene such as hereditary breast cancer (BRCA1 or BRCA2), polyposis coli (APC), Li-Fraumeni syndrome (TP53), and familial retinoblastoma (RB1) are very rare, and most familial cancers seem to be the result of a spectrum of genetic risk in the population, varying continuously from very low to very high, because of the combined effects of dozens or even hundreds of low-penetrance variants in different genes, each with a very small effect. The people at highest risk are those who happen to inherit a large number of such variants. This has been studied most extensively for breast cancer. The high risk in patients’ identical twins indicates that susceptible women contribute a high proportion, and perhaps even the majority, of overall breast cancer incidence. This must be due mainly to low-penetrance genes, as only about 2% of all cases are attributable to inactivating mutations in BRCA1 or BRCA2. Such polygenic susceptibility conferring a site-specific lifetime risk the order of 30–50% in those at highest risk may underlie many cancers. The effects of such variants in combination with each other and with environmental risk factors could be substantial, but their total contribution to cancer incidence will not be known until data on risk factors and extensive genotyping are available for very large numbers of patients and controls. Recent studies have focused on inactivating mutations or polymorphisms in genes involved in cellular mechanisms of cancer development rather than carcinogen metabolism. This is now a major area of research, and several low-penetrance genes have already been discovered. Inactivating mutations in several genes that interact with BRCA1 or BRCA2 (ATM, CHEK2, BRIP1, PALB2) increase the breast cancer risk by approximately twofold, and some polymorphisms in such genes also confer a moderately increased cancer risk. An example is the I1307K single nucleotide polymorphism (SNP) in the APC gene, which is carried by about 1 in 20 Ashkenazi Jews and almost doubles their colon cancer risk.
Genomewide Studies
Complete genetic information on cancer patients and healthy controls will ultimately require sequencing of the whole genome in many thousands of individuals. This is not yet feasible, but a million known SNPs throughout the genome can now be analyzed simultaneously, and verylarge-scale studies involving protein and RNA expression profiles or DNA methylation at specific sites are also being carried out. Genomewide SNP studies have identified common haplotypes (ancient DNA sequences that may be carried by 10% or more of the population) associated with prostate, colorectal, and breast cancer risk. These associations sometimes identify a specific gene, but some are in noncoding regions, and their significance is not yet understood. A SNP that is commoner in cancer patients may cause the specific alteration in a protein that produces the increased cancer risk, but most merely identify a region containing an unknown susceptibility locus, and discovering the relevant sequence variant and its effects may require extensive further research.
Mechanisms Of Carcinogenesis
Age-incidence patterns for non-hormone-dependent carcinomas, and the effects of timing and dose level of various agents alone and in combination (particularly smoking, alcohol, ionizing radiation, and some occupational carcinogens), are parsimoniously explained by the multistage model of carcinogenesis. This was developed many years before the identification of any of the hypothesized sequence of heritable events in human carcinogenesis and has led to several important conclusions, notably the epidemiological and experimental evidence that somatic aging processes per se play little or no role in carcinogenesis (Figure 4).
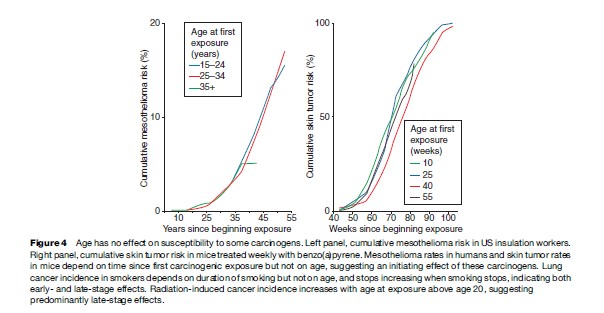
The incidence rate of cancer is presumably proportional both to the rate of the final rate-limiting step in carcinogenesis and to the number of premalignant cells that have undergone all but this final step. The rapid increase in the lung cancer incidence rate among continuing smokers ceases when they stop smoking, the rate remaining roughly constant for many years in exsmokers. The fact that the rate does not fall abruptly when smoking stops indicates that the mysterious final event that triggers the clonal expansion of a fully malignant bronchial cell is unaffected by smoking, suggesting a mechanism involving signaling rather than mutagenesis. Such data are still generating new mechanistic hypotheses.
The Future Of Cancer Epidemiology
Over the next decade, cancer epidemiologists will be increasingly preoccupied with genetically susceptible subgroups. Comparison of the DNA in cancerous and normal cells from the same patient may lead directly to the identification of most of the genes that are commonly mutated in carcinogenesis. Candidate genes are also being identified on the basis of structural homologies from the human genome sequence. Extensive sequence or SNP comparisons between affected relatives and between cancer patients and controls may define combinations of polymorphisms or inherited defects in such genes that identify a few percent of the population whose average lifetime risk may be as high as 50% for a particular cancer. An alternative possibility is that many susceptibility genes will be discovered by studying phenotypic characteristics such as mammographic density or chromosomal instability that correlate with cancer risk. Assays for defective DNA repair correlate consistently with substantially increased susceptibility, and chromosomal aberrations predict increased cancer risk irrespective of carcinogenic exposure.
Once they are identified, susceptible people might benefit disproportionately from screening or prophylaxis, while those at low risk would be reassured. But there will also be penalties. A different susceptible minority will be identified for each disease, and a high proportion of the population may eventually suffer the consequences of being classed as genetically susceptible to some major risk. The hazards of screening for cancer susceptibility are illustrated by the widespread introduction of testing for prostate-specific antigen in the United States, which has reduced prostate cancer mortality only marginally but has led to a sharp increase in recorded incidence and considerable postoperative psychosexual and physical morbidity. Striking gene–environment interactions may be discovered, but most causes of cancer are likely to increase the risk by a smaller amount but a similar factor in those who are less susceptible. If smokers are less likely to stop smoking on discovering that their lifetime lung cancer risk is only 10%, the population death rate might even be increased by such knowledge.
Advances in genetic and molecular understanding will increasingly enable epidemiologists to quantify the relationships between risk factors and specific events in carcinogenesis. Direct monitoring of changes in the genes that underlie carcinogenesis or their products is likely to provide sensitive and specific measures that can be correlated both with cancer incidence and with exposure to carcinogenic agents or activities. Characteristic mutations in DNA from subclinical cancers or their precursor lesions can already be quantified, and serum levels of hormones such as estrogen and prolactin, or growth factors such as insulin-like growth factor-I, as well as chromosomal damage itself, are predictive of increased risk for certain cancers. The effects of some carcinogens are seen mainly in histological subtypes of cancer. For example, smoking increases the risk for squamous cell cervical cancer, but not for the adenomatous type. Such research is now extended through the identification of subtypes of cancer that develop through different pathways by analysis of their patterns of gene alterations or protein expression.
The most significant developments in cancer epidemiology may result from discoveries in virology and tumor immunology. The speculation that unidentified viruses (perhaps including some animal viruses) are associated with many human cancers is consistent with the large increase in overall cancer rates seen in immunosuppressed patients (Buell, 2005). The difficulty is that an unknown virus might mimic the epidemiological effects of dietary or genetic mechanisms. Thus, for example, the migrant patterns for prostate cancer (Figure 2) might be due partly to an endemic infection, as they are for stomach cancer. Viruses usually act synergistically with other carcinogens and therefore provide alternative approaches to risk reduction. The crucial issue is which of the increased cancer risks in immunosuppressed patients reflect an unknown viral etiology and which reflect immunosurveillance targeted at nonviral tumor markers. Some cancers may well be preventable by vaccination with tumor-specific antigens or by some less specific immunostimulation.
Current Priorities In Cancer Prevention
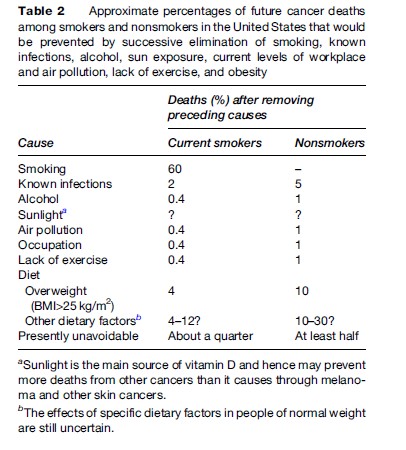
The large differences in the pattern of cancer incidence between developed and developing countries (Figure 1) imply different priorities for prevention, but at an individual level the most important difference is between smokers and nonsmokers, particularly in developed countries. Table 2 shows approximate percentages of future cancer deaths in the United States that would be avoided by successively removing the effects of smoking, known infections, alcohol, current occupational and environmental pollution, inactivity, and obesity. Whether sunlight increases or reduces overall cancer mortality is not yet established. The additional effect of specific dietary recommendations such as those of the American panel (American Institute for Cancer Research/World Cancer Research Fund, 1997) is much more speculative. Avoidance of overweight and prevention or treatment of oncogenic infections are the most important aims for nonsmokers; but it is absurd for smokers in the West to worry about anything except stopping smoking.
Tobacco causes one-third of all cancer deaths in developed countries. About one in five of cancers worldwide are caused by known infectious agents. HBV alone causes almost as many cancers as smoking in China, and can be prevented by vaccination. HPV vaccines may eventually prevent almost all cervical cancers, and if the prevalence of H. pylori can be reduced, many stomach cancers would be avoided. The belated elimination of asbestos by many Western countries will eventually prevent the great majority of mesotheliomas and many lung cancers. Various cancer screening tests are partially effective, and cervical screening is very effective.
Bibliography:
- American Institute for Cancer Research/World Cancer Research Fund (2007) Food, Nutrition and the Prevention of Cancer: A Global Perspective. Washington, DC: American Institute for Cancer Research/World Cancer Research Fund.
- Buell JF, Gross TG, and Woodle ES (2005) Malignancy after transplantation. Transplantation 80: S254–S264.
- Calle EE, Thun MJ, Petrelli JM, Rodriguez C, and Heath CW (1999) Body-mass index and mortality in a prospective cohort of US adults. New England Journal of Medicine 341: 1097–1105.
- Doll R and Peto R (1981) The causes of cancer: Quantitative estimates of avoidable risks of cancer in the United States today. Journal of the National Cancer Institute 66: 1191–1308.
- Doll R and Peto R (2005) Epidemiology of cancer. In: Warrell DA, Cox T, Firth J, and Benz EJ Jr (eds.) (2005) Oxford Textbook of Medicine, 4th edn., pp. 193–218. Oxford, UK: Oxford University Press.
- Greenwald P, Anderson D, Nelson SA, and Taylor PR (2007) Clinical trials of vitamin and mineral supplements for cancer prevention. American Journal of Clinical Nutrition 85: 314S–317S.
- Liu BQ, Peto R, Chen ZM, et al. (1998) Emerging tobacco hazards in China: 1. Retrospective proportional mortality study of one million deaths. British Medical Journal 317: 1411–1422.
- Parkin DM, Bray F, Ferlay J, and Pisani P (2005) Global cancer statistics, 2002. CA: A Cancer Journal for Clinicians 55: 74–108.
- Parkin DM (2006) The global health burden of infection-associated cancers in the year 2002. International Journal of Cancer 118: 3030–3044.
- Peto R, Lopez D, Boreham J, et al. (1994) Mortality from Tobacco in Developed Countries, 1950–2000. Oxford, UK: Oxford University Press.
- Peto R, Watt J, and Boreham J (2006) Deaths from Smoking. Geneva, Switzerland: International Union Against Cancer (UICC).
- Adami H-O, Hunter DJ, and Trichopoulos D (2002) Textbook of Cancer Epidemiology. Oxford, UK: Oxford University Press.
- Buffler PE (1997) Mechanisms of Carcinogenesis: Contributions of Molecular Epidemiology. Lyon, France: International Agency for Research on Cancer.
- Dos Santos Silva I (1999) Cancer Epidemiology: Principles and Methods. 2nd edn. Lyon, France: International Agency for Research on Cancer.
- Peto J, Carbone M (eds.) (2004) Cancer epidemiology. Oncogene 23: 6327–6540
- Schottenfeld D and Fraumeni JF (2006) Cancer Epidemiology and Prevention, 3rd edn. New York: Oxford University Press.
- Stewart BW and Kleihues P (2003) World Cancer Report. Lyon, France: IARC Press.
- https://www.cancer.org/ – American Cancer Society.
- https://www.cancer.gov/ – American National Cancer Institute.
- https://www.cancerresearchuk.org/ – Cancer Research UK.
- https://www.deathsfromsmoking.net/ – Deaths from smoking. Estimates of the number of deaths caused by smoking, for each of 40 developed countries (and five groupings of countries).
- https://www-dep.iarc.fr/ – International Agency for Research Cancer, which includes worldwide cancer incidence and mortality data.
More Cancer Research Paper Examples:
ORDER HIGH QUALITY CUSTOM PAPER

Always on-time

Plagiarism-Free

100% Confidentiality