
Sample Disorders of Impulse Control Research Paper. Browse other research paper examples and check the list of research paper topics for more inspiration. iResearchNet offers academic assignment help for students all over the world: writing from scratch, editing, proofreading, problem solving, from essays to dissertations, from humanities to STEM. We offer full confidentiality, safe payment, originality, and money-back guarantee. Secure your academic success with our risk-free services.
In this research paper we review research and theory across several different conditions that appear to have deficits in impulse control in common. The construct of disorders of impulse control is similar to disinhibitory psychopathology, a term used by Gorenstein and Newman (1980) to refer to a range of conditions across the life span marked by a failure of self-control. The unifying themes across these related yet distinct conditions include deficits in inhibition and excesses in rule-breaking or norm-violating behavior. The paper focuses on a select subset of clinical disorders, specifically substance use disorders and pathological gambling. However, deficits in self-control clearly are important features of some personality disorders (such as antisocial and borderline personality disorders), of childhood disorders such as attention-deficit/hyperactivity disorder and conduct disorder, and of other clinical conditions such as mania, some paraphilias, and what the Diagnostic and Statistical Manual (DSM) of the American Psychiatric Association (APA, 1994) terms impulse-control disorders not elsewhere classified (including intermittent explosive disorder, characterized by discrete episodes of failure to resist aggressive impulses; kleptomania; pyromania; and trichotillomania, characterized by recurrent pulling out of one’s hair for pleasure, gratification, or relief of tension that results in noticeable hair loss).
Academic Writing, Editing, Proofreading, And Problem Solving Services
Get 10% OFF with 24START discount code
In addition to reflecting a failure of impulse control (i.e., a tendency to engage in the behavior despite attempts or desires to resist), we could also characterize these disorders as indicating excessive appetite (i.e., a strong underlying drive toward engaging in the behavior; Orford, 2001). Orford proposes that the core central processes underlying conditions such as alcohol dependence, drug dependence, nicotine dependence, pathological gambling, excessive eating, and sexual addiction are related to both “deterrence and restraint” and “primary, positive incentive learning mechanisms” (pp. 19–20). That is, these disorders might be viewed as conditions resulting from a conflict between inclination and inhibition, and an adequate conceptualization of the problem places emphases on both the compelling and the restraining (i.e., inhibitory) aspects of the phenomenon.
Disinhibition
Although it is not unusual for psychologists to discuss impulsivity and inhibition as unitary constructs, it is clear that they are not. For example, impulsivity has been operationalized in myriad ways and some alternative measures of impulsivity are not highly correlated (e.g., White et al., 1994). In a probing review, Nigg (2000) distinguishes eight specific forms of inhibition described by psychologists, each with different functional relations to behavior and neurological substrates. Probably of greatest relevance for understanding disorders of impulse control are those inhibition systems related to socalled behavioral inhibition (e.g., suppression of prepotent responses), response to punishment cues, and response to novelty.
Prior to discussing individual disorders we first consider evidence supporting the hypothesis that there is a broad class of disorder sharing a common factor of disinhibition. This evidence stems from studies showing both high cooccurrence (i.e., comorbidity) of ostensibly different disorders and common etiologically relevant correlates.
Comorbidity Among Impulse Control Disorders
The categorical approach to diagnosis exemplified by the DSM (versions III, III-R, and IV) of the APA (1980, 1987, 1994) is predicated upon the idea of distinct diagnostic entities. Although similarities among disorders can be represented by membership in the same class or subclass of a hierarchical diagnostic system, disorders are still represented as distinct entities. Within the tradition of the DSM, high cooccurrence between two disorders (i.e., comorbidity) suggests the possibility that the two disorders are members of the same general class of disorders. An alternative approach to classification is the factor-analytic approach whereby varying forms and degree of psychopathology are represented as dimensional constructs and an individual’s symptomatology can be represented as a score on multiple dimensions. Although there is considerable debate regarding whether psychopathology is best represented as distinct classes or multiple dimensions (Klein & Riso, 1993; Widiger, 1997), both categorical and dimensional approaches indicate high comorbidity.
For example, in one large epidemiological study (Kessler, Crum, Warner, & Nelson, 1997), the diagnosis of alcohol dependence was strongly associated with other disorders characterized by disinhibition (e.g., conduct disorder, antisocial personality disorder, drug use disorders, and mania) as well as disorders for which affective disturbance is the cardinal feature (e.g., anxiety and depressive disorders). This high comorbidity could suggest either shared etiological processes or that the presence of one of these disorders increases the likelihood of developing a second disorder. (It is also possible that overlap in the diagnostic criteria could be responsible as well.) Regardless of the underlying mechanism, comorbidity among disorders of impulse control is common and implies some form of causal mechanism related to inhibitory processes.
However, some ostensible comorbidity might merely represent short-term, transient psychiatric disturbances induced by acute substance intoxication or by a withdrawal syndrome that mimics independent disorders. In the DSM-IV, criteria are set out for a number of substance-induced disorders (e.g., substance-induced mood disorder, substanceinduced psychotic disorder). The issue is more than academic; the course and treatment implications of substance-induced and independent disorders are quite different because substance-induced disorders are, by definition, likely to remit or improve after a prolonged period of abstinence (Kadden, Kranzler, & Rounsaville, 1995; Schuckit, 1994). Attribution of substance induction might be straightforward in some cases, as with, for example, an alcohol dependent individual whose depression remits within a couple of weeks of detoxification (and whose depression never occurs during prolonged period of sobriety). However, in many cases, determining whether conditions such as anxiety disorders, mood disorders, and psychotic disorders are independent or substance induced can be difficult in practice, especially when a substance use disorder and another condition have coexisted for many years, have insidious onsets, or have fluctuating courses. Moreover, by early adolescence there is often cooccurrence of symptoms (e.g., negative affect and drinking) prior to any morbidity in a formal diagnostic sense (Costello, Erkanli, Federman, & Angold, 1999). Thus, although useful conceptually and clinically, the distinction between independent and substance-induced disorders can sometimes be problematic.
In childhood and adolescence, there is considerable evidence for the existence of a broad class of symptomatology usually labeled as externalizing disorders. Almost 25 years ago, Achenbach and Edelbrock (1978) reviewed the empirical literature on the structure of childhood behavior problems and concluded there was consistent evidence for two broadband factors of psychopathology, which they termed overcontrolled and undercontrolled. The broadband undercontrolled factor subsumed behaviors labeled as “aggressive, externalizing, acting out, [and] conduct disorder” (p. 1284), which suggests that these problems may share some common features. Subsequent research has strongly supported the validity of the broadband factor of undercontrolled behavior, now usually referred to as externalizing behavior, which represents a higher order factor subsuming delinquent and aggressive behavior (see Achenbach, 1995). Additional factor-analytic studies of samples of adolescents and young adults by Jessor and his colleagues (Donovan & Jessor, 1985; Donovan, Jessor, & Costa, 1988; Jessor, Donovan, & Costa, 1991) offer strong support for a broad class of problem behaviors indicated by problem drinking, marijuana use, other illicit drug use, cigarette smoking, and what they termed general deviant behavior (e.g., vandalism, fighting, theft). They labeled this factor the syndrome of problem behavior while acknowledging that there is considerable unique variability in each of the problem behaviors that is not accounted for by the general problem-behavior factor.
The construct of a broadband externalizing factor appears to generalize to adults. Krueger (1999; Krueger, Caspi, Moffitt, & Silva, 1998) provided evidence of this from two different studies employing structured diagnostic interviews (a nationally representative survey of mental disorders in the United States, and a New Zealand birth cohort studied prospectively from age 18 to age 21). Factor analyses of diagnoses from both studies offered strong support for a broadband externalizing psychopathology factor indicated by alcohol dependence, drug dependence, and antisocial personality disorder, and this externalizing factor showed high temporal stability over a 3-year interval.
Overall, there appears to be strong evidence for the view that covariation among symptoms of substance use disorders and general antisociality can be modeled as reflecting a higher order factor indicative of externalizing psychopathology or behavioral undercontrol (see also Zuckerman, 1999) suggesting that these correlated disorders may share common, core etiological processes. In principle, identification of these core processes would provide support for the validity of the construct of externalizing psychopathology and would also provide a foundation for identifying factors that are unique to individual disorders.
Common Childhood Correlates
Conditions such as substance use disorders, pathological gambling, and antisocial behavior have their roots in childhood and adolescence. To the extent that there is some degree of developmental continuity, common childhood precursors are strongly implied. For example, childhood antisocial behavior and poor parental monitoring are common precursors of adult antisocial behavior, early alcohol involvement, and drug involvement (for reviews see Caspi & Moffitt, 1995; Dishion, French, & Patterson, 1995; Zucker, Fitzgerald, & Moses, 1995). This is not to say that these different outcomes are functionally the same, only that there appears to be an overlap of etiological factors. Longitudinal, behavior geneticfindings can help shed further light on the nature of common etiological antecedents. For example, in a study of adults, Slutske et al. (1998) showed a strong genetic correlation between childhood conduct disorder and alcohol dependence, indicating that much of the overlap between these disorders is due to common genetic influences and that genetic variation in the personality dimension of behavioral undercontrol (impulsivity, interpersonal exploitativeness, and social nonconformity) can explain nearly all of this common underlying genetic predisposition (Slutske et al., 2002). Such studies of the genetic causes of comorbidity would help to further identify underlying, heritable dimensions or traits contributing to the range of impulse-control disorders.
Personality Correlates
The assumption that disorders of impulse control are related at the level of personality is implicit in much clinical thinking and is explicit in some older diagnostic schemes (DSM-I; APA, 1952). Influential theorists (e.g., Cloninger, 1987a, 1987b; Gorenstein & Newman, 1980) have postulated a common underlying vulnerability to multiple disorders associated with disinhibition. Indeed, Cloninger (1987a, 1987b) proposes an identical configuration of personality traits underlying both a subtype of alcohol dependence and antisocial personality disorder (APD).
In recent reviews of the personality literature on alcoholism and APD (Sher & Trull, 1994) and on alcoholism and other substance use disorders (Sher, Trull, Bartholow, & Vieth, 1999) we have arrived at similar conclusions: There are consistent patterns of association between certain broadband personality characteristics (specifically, impulsivity and neuroticism) and a wide range of externalizing psychopathology. Research on the personality correlates of pathological gambling (PG) is not as well developed as it is for substance use disorders, with most studies of PG based upon small samples of patients in treatment. For example, there are no studies of the personality correlates of those at high versus low risk for the development of PG, and very limited relevant prospective data. Despite the lack of strong empirical foundations, theories of the etiology of PG implicate the personality dimensions of neuroticism–negative emotionality (e.g., Dickerson & Baron, 2000; Hand, 1998) and impulsivity-disinhibition (e.g., Dickerson & Baron, 2000) as important risk factors for the subsequent development of PG. Moreover, existing studies are generally consistent in demonstrating a pattern of personality correlates for PG similar to what has been obtained for the substance use disorders. Individuals in treatment for PG have elevated levels of neuroticism–negative emotionality (Blaszczynski, Buhrish, & McConaghy, 1985; Blaszczynski, Steel, & McConaghy, 1997; Blaszczynski, Wilson, & McConaghy, 1986; Ciarrocchi, Kirschner, & Fallik, 1991; Graham & Lowenfeld, 1986) and impulsivity-disinhibition (Blaszczynski et al., 1985, 1986, 1997; Ciarrocchi et al., 1991; Graham & Lowenfeld, 1986; McCormick, Taber, Kruedelbach, & Russo, 1987; Steel & Blaszczynski, 1998) compared to unaffected controls. The results for extraversion-sociability are mixed, with some studies failing to find an association with PG (Blaszczynski et al., 1985, 1986; Ciarrocchi et al., 1991; Graham & Lowenfeld, 1986), and with others finding either a positive association (McCormick et al., 1987) or a negative association (Blaszczynski et al., 1997).
Neuroticism–Negative Emotionality
Findings from several major longitudinal studies of substance use disorders do not suggest a strong causal role for neuroticism–negative emotionality (e.g., Jackson, Sher, & Wood, 2000; Jones, 1968; Robins, Bates, & O’Neal, 1962; Sher, Bartholow, & Wood, 2000; Vaillant & Milofsky, 1982). In contrast, other prospective studies do implicate negative emotionality as predictive of later alcohol involvement (Caspi et al., 1997; Chassin, Curran, Hussong, & Colder, 1996; Cloninger, Sigvardsson, Reich, & Bohman, 1988; Labouvie, Pandina, White, & Johnson, 1990; Sieber, 1981). However, it should be noted that Cloninger et al. specify that low negative affectivity (characterized by low scores on the Harm Avoidance scale of the Tridimensional Personality Questionnaire [TPQ], Cloninger, 1987c) is most relevant to the development of early-onset alcoholism, whereas people high in negative affect are susceptible to the occurance of alcohol dependence later in life.
This divergent pattern of findings indicates that our understanding of the role played by neuroticism–negative emotionality in substance use disorder is far from complete, particularly given that the existing database of informative prospective studies remains relatively sparse. Furthermore, the issue may be best resolved by considering moderating variables influencing the relationship between negative emotionality and substance use (e.g., Greeley & Oei, 1999; Sher, 1987).
Impulsivity-Disinhibition
The broad personality dimension that appears to be most relevant to impulse-control disorders is that of impulsivitydisinhibition. This dimension incorporates traits such as sensation seeking, aggressiveness, impulsivity, and psychoticism, and has been termed impulsive, undersocialized sensation-seeking by Zuckerman (1994). The high rates of comorbidity between alcohol use disorders and both antisocial and borderline personality disorders (discussed later) provide support for the idea that clinical alcoholics tend to be impulsive (e.g., Regier et al., 1990), and alcoholics tend to score high on psychometric measures assessing this dimension (e.g., Bergman & Brismar, 1994; Plutchik & Plutchik, 1988). Moreover, alcoholics with comorbid APD experienced a more severe and chronic course of alcoholism, and engaged in more drug use, compared to those without this comorbid diagnosis (e.g., Holdcraft, Iacono, & McGue, 1998).
Additionally, cross-sectional high-risk studies (e.g., Alterman et al., 1998; Sher, 1991) demonstrate that traits reflecting impulsivity-disinhibition are elevated in the offspring of alcoholics. Most importantly, prospective studies consistently indicate that impulsive-disinhibited individuals are at elevated risk for the development of substance-related problems (e.g., Bates & Labouvie, 1995; Caspi et al., 1997; Cloninger et al., 1988; Hawkins, Catalano, & Miller, 1992; Pederson, 1991; Schuckit, 1998; Sher et al., 2000; Zucker & Gomberg, 1986; Zucker et al., 1995). Although there are no prospective studies of personality and PG, Vitaro, Arsenault, and Tremblay (1997) found that a five-item self-report measure of impulsiveness completed at age 13 predicted gambling problems at age 17 among 754 boys. Additionally, in a subsample of 154 boys it predicted gambling problems even after controlling for socioeconomic status, frequency of gambling involvement at age 13, and measures of anxiety and aggressiveness (Vitaro, Arsenault, & Tremblay, 1999). The importance of impulsivity-disinhibition as an early predictor of later alcohol problems has been outlined in detail by Zucker et al. (1995). These authors hypothesize that the prospective relation between childhood impulsivity-disinhibition (or childhood conduct disorder) and later drinking problems marks an etiologic process whereby these traits lead to poor school performance and relational problems. These troubles in turn may lead such individuals to associate with similar peers, who are likely to begin using alcohol and other drugs early in adolescence. Moreover, conduct disorder and alcohol dependence have been linked to the influence of genes that increase the risk for both disorders (Slutske et al., 1998).
Because it has been argued that antisociality reflects merely behavior and not personality as defined by classic personality theorists (see Nathan, 1988), studies demonstrating that personality variables can statistically explain the relation between antisocial behavior and alcoholism can be of theoretical relevance. In one such study, Earleywine and Finn (1991) demonstrated that the cross-sectional relation between alcohol use and a scale that heavily samples antisocial behavior can be statistically explained by the effect of sensation seeking on both variables. Stronger support for a common underlying vulnerability related to personality traits is provided by Jang, Vernon, and Livesley (2000), who found some common genetic influence upon alcohol misuse and personality traits related to antisociality (specifically sensation-seeking, recklessness, and impulsivity) as well as to narcissism (grandiosity and attention seeking), and by Slutske et al. (2002), who found that about 40% of the genetic susceptibility for alcohol dependence was shared with genetic variation in the personality dimension of behavioral undercontrol (impulsivity, interpersonal exploitativeness, and social nonconformity). It would be useful to extend these types of analyses to a broader range of impulse-control disorders.
Extraversion-Sociability
The evidence concerning the relationship between extraversion-sociability and impulse-control disorders can best be described as mixed. Most reviews of the clinical literature (e.g., Barnes, 1983; Cox, 1987) do not suggest that, as a group, individuals with substance use disorders differ from controls on the dimension of extraversion-sociability, although as dependence becomes severe, levels of extraversionsociability may decrease (Rankin, Stockwell, & Hodgson, 1982). Moreover, high-risk, cross-sectional studies do not typically indicate that children of alcoholics differ from controls on this trait (Sher, 1991), although sociability predicted substance use for adolescent children of alcoholics but not for controls in one study (Molina, Chassin, & Curran, 1994). On the other hand, at least one other recent cross-sectional study did not find a significant relationship between extraversion and either alcohol use frequency or alcohol problems using a nonclinical sample (Stacy & Newcomb, 1998). However, prospective studies have noted the possibility that extraversion-sociability may be etiologically relevant to the development of substance use problems. For example, Jones (1968) reported that prealcoholics were rated as being high in expressiveness and gregariousness. Also, sociability has been found to prospectively predict frequency of intoxication (Sieber, 1981). Another, more recent prospective study found that higher extraversion scores predicted alcohol dependence among young adults over a 3.5-year interval (Kilbey, Downey, & Breslau, 1998).
There may be more consistency in the mixed patterns of findings than appears on the surface. For example, it seems possible that extraversion-sociability is a risk factor for the development of substance involvement (especially because substance initiation usually occurs in a social context), and that this trait becomes increasingly masked in those whose levels of dependence increase over time. Another possibility is that other third variables may play a role in determining the influence of extraversion on substance use disorders. For example, some recent evidence suggests a gender difference wherein high extraversion scores may be more relevant for predicting alcohol problems in women than in men (e.g., Heath et al., 1997; Prescott, Neale, Corey, & Kendler, 1997). Furthermore, it is currently unclear whether these outgoing characteristics most accurately reflect true sociability or (misattributed) disinhibition (Tarter, 1988). Additional systematic investigations of this association with prospective data, including consideration of other potential moderating and mediating processes, would prove helpful in better identifying the importance of traits related to extraversion.
Common Biological Substrates
There is a scattered but large literature linking biological variables to individual differences in the trait of impulsivity in general and to disorders of impulse control in particular (Zuckerman, 1991). Note that because of acute and chronic effects of psychoactive substances on the individual, it can be very difficult to attribute differences in brain function to a predisposing vulnerability versus a consequence of substance use (e.g., Hare, 1984).
One of the most actively researched questions currently is whether deficits in so-called executive functioning (e.g., planning, organizing, selective attention, some forms of inhibitory control) are related to disorders of impulse control. Because these functions are associated with activity located in the frontal cortex (Luria, 1980; Stuss & Benson, 1985), they are sometimes described as frontal functions. However, because of extensive connections between the frontal lobes and other brain regions, localization of any complex executive function is probably an oversimplification. Hypofrontality (i.e., decreased frontal lobe activity) and related impaired executive functions have been hypothesized to be related to certain forms of impulsivity in general (e.g., Nigg, 2000), conduct disorder, and adult antisocial behavior and substance use disorders (e.g., Gorenstein, 1987). In a recent metaanalysis, Morgan and Lilienfeld (2000) reported an overall negative association between executive functions and antisociality across a variety of ages and populations. Children of alcoholics, who are at high risk for a range of disorders of impulse control (esp. substance use disorders), have been shown to have a range of cognitive deficits, some of these related to executive functions (Pihl & Bruce, 1995; Polich, Pollock, & Bloom, 1994; Sher, 1991). Although, to date, the neuropsychology of pathological gamblers has not been well studied, there have been recorded cases of the development of PG subsequent to frontal lobe injury (Blaszczynski, Hyde, & Sandanam, 1991). Thus there are a number of converging findings suggesting that deficits in cognitive functions subsumed under the rubric of executive control relate to a range of disorders of impulse control. However, much of the primary literature is characterized by serious design limitations: There is great variability among researchers in how various cognitive functions are classified; the specificity to executive functions (as opposed to nonexecutive functions) is not always clear; and some disorders not typically thought of as disorders of impulse control (e.g., schizophrenia, obsessive-compulsive disorder) may also be associated with similar deficits. Thus, there is a need for studies bringing a higher degree of resolution in relating specific forms of neurocognitive deficits to specific symptoms and syndromes.
Impulsivity and associated disorders have also been associated with several distinct neuropharmacological systems, in particular the serotonin, dopamine, and norepinephrine systems (Zuckerman, 1991). Many of these studies have sought to establish correlations between the presence of a disorder (e.g., alcohol dependence; Major & Murphy, 1978; PG; Blanco, Orensanz-Munoz, Blanco-Jerez, & Saiz-Ruiz, 1996) or variations in a personality trait (e.g., sensation seeking; Schooler, Zahn, Murphy, & Buchsbaum, 1978) and differing levels of neurotransmitter metabolites or enzymes responsible for neurotransmitter metabolism. Other studies have employed acute pharmacological challenges in order to alter the functioning of a neurotransmitter system (e.g., LeMarquand, Benkelfat, Pihl, Palmour, & Young, 1999) and examine the effect on impulsive behavior. Additionally, treatment outcome studies of impulse-control disorders investigating medications known to have effects on specific neurotransmitter systems (e.g., selective serotonin reuptake inhibitors, or SSRIs) have relevance to understanding the biological bases of these conditions.
Research on biological markers of impulsivity and associated disorders has been going on for more than 20 years, and numerous intriguing findings implicate functionally high levels of dopaminergic activity and low levels of noradrenergic and serotonergic activity (Zuckerman, 1991, 1999) in impulsivity and in disorders of impulse control. However, it is difficult to point to many results that implicate a robust, specific deficit. For example, although low serotonergic activity is posited to play a role in substance use disorders, clinical outcome trials of SSRIs have had inconsistent results (Litten & Allen, 1998).Additionally, a low level of monoamine oxidase (an enzyme important in the breakdown of dopamine, norepinephrine, and serotonin) activity is claimed to be “one of the most reliable biological markers for sensation seeking and impulsivity traits and disinhibitory disorders such as [APD], alcohol and substance abuse, and other disorders characterized by poor impulse control . . . [including PG]” (Zuckerman, 1999, p. 309). However, the association often is small and it is possible, if not likely, that even this relationship is an artifact of comorbid tobacco use (Anthenelli et al., 1998; Sher, Bylund, Walitzer, Hartmann, & Ray-Prenger, 1994).
Given heterogeneity within primary diagnostic groups, it is possible that strong relations between disorders and biological markers are obscured by mixtures of disorder subtypes. For example, Linnoila, Virkkunen, George, and Higley (1993) review evidence suggesting that although early-onset alcoholism is characterized by low levels of serotonin metabolites in cerebrospinal fluid, later onset alcoholism is not; and this early versus late onset maps onto a distinction between more and less impulsivity (e.g., see discussion of alcoholism typologies later in this research paper). Pettinati et al. (2001) reported that sertraline (a specific serotonin reuptake inhibitor) was effective at reducing drinking in alcoholics without a history of depression. It seems fair to say that we are still at an early stage of understanding the neuropharmacological foundation of impulsivity and related disorders. Presumably, progress in behavioral genomics (which will identify specific genes associated with specific biological processes) will help guide the next leg of this important research direction.
Substance Use Disorders and Pathological Gambling
In the following sections, we focus on three disorders of impulse control: (a) alcohol use disorders, (b) drug use disorders, and (c) pathological gambling. As operationalized by the DSM-IV, these conditions share in common a number of features, including preoccupation with engaging in the behavior (i.e., either substance use or gambling); inability to abstain from the behavior; tolerance (e.g., either using more of a substance or increasing the stakes in gambling to get the desired effect); and withdrawal (e.g., discomfort or irritability when abstaining from the behavior). Although each of these disorders have unique features (e.g., PG’s chasing losses) their underlying commonalities permit a more indepth analysis of basic mechanisms likely common to a number of conceptually distinct conditions.
Before separately discussing alcohol use disorders and drug use disorders, we first consider the concepts of substance abuse and substance dependence. The abuse-dependence distinction is applicable to both alcohol use and drug use disorders, and dependence-related concepts are increasingly being applied to other conditions such as PG and other types of addictive behaviors (e.g., so-called sexual addiction, Internet addiction).
The Abuse and Dependence Syndromes
Most theory and research on the distinction between abuse and dependence has been targeted on the use of alcohol, and so our discussion will focus on this substance. More than 150 years ago, the term alcoholism was introduced by Magnus Huss to indicate a condition resulting from excessive consumption of alcohol (Keller & Doria, 1991). Subsequently, alcoholism has been alternately construed as any use of alcohol that negatively affects the drinker or society (Jellinek, 1960), as a syndrome of problem drinking (ICD-8; World Health Organization [WHO], 1967), as a personality disorder (DSM-I;APA, 1952), or as a disease marked by signs of physiological adaptation (e.g., tolerance or withdrawal) or loss of control over drinking (Feighner et al., 1972; National Council on Alcoholism [NCA] Criteria Committee, 1972). Eventually, classification systems formally contrasted dependence on alcohol with alcohol abuse—a pattern of maladaptive alcohol use characterized by negative social, legal, or occupational consequences (DSM-III;APA, 1980). In this way, the hazardous use of alcohol was contrasted with a more severe form of dependency on alcohol characterized by physiological symptoms.
Early operationalizations of alcohol dependence, such as the DSM-III (APA, 1980), NCA Criteria Committee (1972), and the World Health Organization (1967) criteria for alcohol dependence, required evidence of physiological dependence, indicated by tolerance or withdrawal. At about the same time the NCA and DSM-III criteria were being drafted, Edwards and Gross (1976) proposed an alternate dependence concept, the Alcohol Dependence Syndrome (ADS), in which physiological signs and symptoms of dependence were indicators of but not necessary criteria for the diagnosis of dependence. Edwards and Gross’s conception of alcohol dependence referred to a syndrome composed of a variety of signs and symptoms that signified the importance that alcohol consumption plays in the life of the drinker. These signs and symptoms include what Edwards (1982, 1986; Edwards & Gross) described as “a narrowing of the drinking repertoire”; centrality of drinking in the person’s life relative to other life tasks and responsibilities; tolerance and withdrawal; “awareness of the compulsion to drink”; and rapid reinstatement of dependence symptoms after a period of abstinence. The broadened construct of dependence introduced by Edwards and Gross was clearly influential in later revisions of the DSM, and symptoms of tolerance or withdrawal were no longer required for the diagnosis of substance dependence in DSM-III-R (APA, 1987) and DSM-IV (APA, 1994; note, however, that “with physiological dependence” remains a specifier of a subtype of dependence in the present DSM).
Edwards (1986) was careful to distinguish alcohol dependence from alcohol-related consequences (or disabilities). Alcohol-related consequences refer to a variety of negative life events that are directly the result of alcohol consumption. These consequences include social problems (e.g., physical or verbal aggression, marital difficulties, loss of important social relationships), legal problems (e.g., arrests for driving while intoxicated, public inebriation), vocational problems (e.g., termination from employment, failure to achieve career goals), and medical problems (e.g., physical injury, liver disease, central nervous system disease). Both substance-related consequences and the dependence syndrome can be viewed as dimensional constructs that can be graded in intensity from absent to severe and do not explicitly reference the amount of substance consumed as a criterion.
The DSM-IV describes two major categories of substance use disorder, specifically substance abuse and substance dependence, that roughly correspond to Edwards and Gross’s (1976) distinction between alcohol-related disabilities and the alcohol dependence syndrome. Within DSM-IV, substance dependence is the more severe disorder and its presence (or its history) excludes the diagnosis of substance abuse.
Factor analysis of alcohol symptom scales in clinical samples of alcoholics tend to suggest a multidimensional structure with at least one factor representing dependence (e.g., Skinner, 1981; Svanum, 1986), but factor analyses employing population-based samples paint a less clear-cut picture. More specifically, mixed abuse and dependence indicators can be well represented by a single factor (e.g., Hasin, Muthen, Wisnicki, & Grant, 1994). When evidence for more than one factor is found, the item content of the factors are not consistent with the DSM criteria sets (e.g., Muthen, Grant, & Hasin, 1993) for separate abuse and dependence symptoms. Moreover, when multiple dimensions are empirically identified, correlations among the factors appear to be exceptionally high, calling into question the value of a multidimensional approach (e.g., Allen, Fertig, Towle, & Altschuler, 1994; Hasin et al., 1994).
Recently, some investigators have begun to question the broadening of the dependence construct that took place in the transition from DSM-III to DSM-III-R, and argue for a narrower definition based on physiological dependence. For example, Langenbucher et al. (2000) propose a withdrawal gate model in which the symptom of withdrawal is both necessary and sufficient for the diagnosis of dependence. Withdrawal-based dependence diagnoses were found to be more reliable and proved to show a stronger pattern of validity along diverse criteria than DSM-IV-based dependence diagnoses. Schuckit et al. (1998) also endorsed the importance of physiological dependence (especially withdrawal) as being an important severity indicator, as evidenced by its association with a range of clinical variables (both psychiatric and substance related). Thus, recent work indicates that substance withdrawal is particularly important clinically and suggests that it should be considered for special attention in future diagnostic revisions. Because this symptom is fairly rare in both adolescent samples (Langenbucher et al., 2000) and nonclinical samples (Helzer, Burnam, & McEvoy, 1991), prevalence estimates of withdrawal-based dependence diagnoses would likely be much lower in both clinical adolescent samples and in nonclinical samples than is currently reported using DSM-III-R and DSM-IV criteria. In typological research using latent-class analysis (a multivariate technique designed to uncover latent classes underlying a set of observations), withdrawal symptoms typically are found only in the most severe subtype of alcohol dependence identified. This appears to be true in both clinical (Bucholz, Heath, Reich, & Hesselbrock, 1996) and nonclinical samples (Heath, Bucholz, Slutske, & Madden, 1994; Nelson, Heath, & Kessler, 1998).
It is unclear why the other putative indicator of physiological dependence, tolerance, has not been found to be as important an indicator of dependence; both tolerance and withdrawal are thought to reflect neurological adaptations related to chronic use. One possibility is that current questionnaireand interview-based assessments of tolerance that rely upon subjective inferences concerning changes in drug sensitivity over time are of limited validity. O’Neill and Sher (2000) found that the course of subjective reports of tolerance over time, in young adulthood, did not conform to prediction (e.g., self-reported tolerance appeared to decrease during young adulthood, even among consistent heavy drinkers). Thus, it may be that current assessment strategies for tolerance are limited and conclusions regarding the importance of tolerance as a dependence criterion await improved assessments of tolerance.
Moving beyond the issue of assessment, research on behavioral aspects of tolerance over the past 35 years has highlighted the role of nonpharmacological factors in tolerance development and expression and, in doing so, has downplayed the concept of tolerance as one of simple neuroadaptation to a psychoactive substance (Siegel, Baptista, Kim, McDonald, & Weise-Kelly, 2000). Siegel and his colleagues have repeatedly demonstrated that conditioned compensatory responses (i.e., opposite in direction to the unconditioned response) to drug effects develop over repeated administrations of a drug along with its associated stimuli (e.g., beverage taste, hypodermic needle, social setting). Over time, these associated stimuli become capable of eliciting conditioned compensatory responses that counteract the direct effects of the drug. Thus, tolerance can be highly situational or context dependent. Consequently, use of a drug in novel circumstances (that lack the situational cues that elicit conditioned compensatory responses) can result in an escape from tolerance (and perhaps even overdose). These situational tolerance effects have been noted for a range of psychoactive substances including opiates, alcohol, and caffeine (Siegel et al.). Such associative processes might be used to explain tolerance for nonpharmacological stimuli such as gambling (e.g., the need to gamble with increasing amounts of money in order to achieve the desired excitement). Siegel andAllen (1998) have shown how nonpharmacological processes, such as the visual-aftereffect phenomenon known as the McCollough effect, appear to involve conditioned compensatory responses; this suggests that conditioning plays a role in a range of homeostatic adjustments, not just those involving drugs.
Similar to Siegel and colleagues’(2000) associative theory of tolerance is a nonassociative theory proposed by Solomon and Corbit’s (1974) opponent-process theory. According to this theory, a positive (or negative) hedonic state (or A-state) elicits a countervailing negative (or positive) hedonic state (or B-state) that serves to counteract the initial state as part of a natural homeostatic mechanism. Over time, the B-state is thought to strengthen, thereby reducing the reaction to the drug (i.e., the opponent B-state reduces the initialA-state). In this way, tolerance is thought to develop. Koob and colleagues (e.g., Koob & Le Moal, 2001) have extended opponent-process theory to account for changes in homeostatic set-point, or allostasis. That is, over time, there is a change in the natural homeostatic set-point so that the B-state no longer balances the evoking A-state and actually serves to overshoot the initial homeostatic set-point. This type of allostatic derangement is thought to characterize chronic dependence, and this deviation from the (original) natural setpoint to the allostatic set-point is believed to represent significant cost to the individual. That is, according to this model, chronic adaptive changes to drug taking dynamically resets homeostatic mechanisms altering the basic hedonic set-point. From this perspective, but also from conditioning models such as Siegel’s, withdrawal phenomena can be viewed as opponent processes acting in the absence of reward and involving the same underlying brain systems (albeit in the opposite direction). It is for this reason that resumption of drug intake (initiating a new A-state) counteracts withdrawal.
In general, the concepts of tolerance and neuroadaptation suggest that many problem behaviors may escalate over time, leading to greater problem involvement. Although the focus on impulse-control disorders is on notions of inclination and inhibition, it may be fruitful to determine the extent that both acute and chronic homeostatic adjustments to the effects of reward tend to maintain these disorders.
Alcohol Use Disorders
Pathological alcohol use is both prevalent and costly in North America and represents a serious health threat in many other developed and developing nations (Helzer & Canino, 1992).
It bears noting that much of the societal cost of alcohol consumption (e.g., unintended injury, motor vehicle crashes) is attributable to the large proportion of individuals who do not necessarily suffer from an alcohol use disorder (AUD), abuse, or dependence, but who do misuse alcohol on occasion. Consequently, effective prevention of alcohol-related harm needs to be broadly based and not targeted only at those withAUDs (Institute of Medicine, 1990; Kreitman, 1986).
History and Evolution of the Concept of Alcoholism
“Alcoholic beverages have been known to almost all people from before the dawn of history” (Poznanski, 1959, p. 42). Seneca (4 B.C.–65 A.D.; 1942) distinguished between two distinct definitions of the word drunken, one definition referring to someone who is acutely intoxicated and poorly selfcontrolled, and the other to someone who is a habitual drinker and “a slave to the habit.” As was true for many psychological disorders, it was during the nineteenth century that leading European physicians attempted to define and describe the condition we now call alcohol dependence.
Perhaps the best known early scholar in the area of alcohol dependence was Magnus Huss, who is credited with creating the term chronic alcoholism and who noted that there was little in the way of a clear boundary between this condition and other mental disorders. However, most modern conceptions of alcohol dependence are more closely associated with the writings of E. M. Jellinek (1960; Bowman & Jellinek, 1941) who described five varieties of alcoholism based on the configuration of etiological elements, alcohol process elements (including both symptom profile and the nature of symptom progression), and the nature of damage. Over the past century, clinicians and researchers have proposed a number of additional typologies (see Babor, 1996) based on a variety of criteria including personality characteristics, drinking patterns, developmental course, heritability, age of onset, and psychiatric comorbidity. Although these various typologies differ in number and kind of types proposed, there appears to be consistent evidence for at least two types.
One type frequently described involves comorbid antisocial tendencies and early onset—for example, Babor et al.’s Type B (1992); Cloninger’s Type 2 (1987a); Knight’s essential (1938); and Zucker’s antisocial (1987). The other type involves later onset and more negative affectivity—for example, Babor et al.’s Type A (1992); Cloninger’s Type 1 (1987a); Knight’s reactive (1938); and Zucker’s negative affect (1987). Still, the value of subtyping alcohol dependence into two or more discrete types remains to be definitively established. Such typologies invariably represent prototypic cases and many affected individuals fail to fit clearly into a single subtype. Moreover, the association between alcohol dependence and subtyping variables such as antisociality (and presumably others, such as age of onset) appears to be graded across the range of levels of antisociality (Sher, 1994), and it is not only high levels of antisociality that are associated with alcohol-related difficulties. Regardless of whether one subscribes to a categorical or dimensional approach with respect to conceptualizing AUDs, there is little question that there is significant heterogeneity with respect to etiological factors, symptoms, and course.
Epidemiology
Over the past 20 years, three large-scale, population-based epidemiological surveys using structured diagnostic interviews have provided estimates of AUDs in the United States. These include the Epidemiologic Catchment Area (ECA) Survey (Helzer et al., 1991; Robins, Bates, & O’Neal, 1991); the National Comorbidity Survey (NCS; Kessler et al., 1994, 1997); and the National Longitudinal Alcohol Epidemiologic Survey (NLAES; Grant, 1997; Grant & Pickering, 1996; Grant et al., 1994). Both the NCS and NLAES employed nationally representative samples that provide a scientific basis for generating prevalence estimates for the United States.
Each of these major studies indicates very high past-year and lifetime prevalences of AUDs in the U.S. population (13.8% lifetime and 6.8% past-year DSM-III in ECA; 23.5% lifetime and 7.7% past-year DSM-III-R in NCS; and 18.2% lifetime and 7.41% past-year DSM-IV in NLAES). Additionally, each of these studies documented that AUDs are most prevalent in men and in young adulthood; dependence is more prevalent than abuse in the NCS and NLAES.
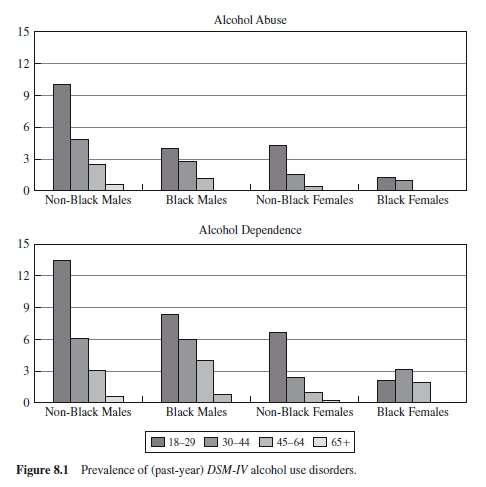
Focusing on the NLAES data (because of that survey’s size and its use of the DSM-IV), we note several important findings that help characterize the relation between AUDs and important demographic variables. First, AUDs are more than twice as prevalent in men than in women, with larger sex differences in older cohorts than in younger cohorts (e.g., AUDs are 4.4 times as prevalent in men vs. women in the 65 age group, but only 2.2 times as prevalent in men vs. women in the 18–20 age group; Grant et al., 1994). Also, alcohol dependence is lower in Blacks than in Whites and Hispanics, and is lower among those who are married and who have higher family incomes (Grant, 1997).
Examination of Figure 8.1 shows how strongly agegraded AUDs (especially alcohol dependence) are in the NLAES study. With the exception of Black women (who tend to have comparatively low rates of alcohol dependence in early adulthood), there is a steep, negative prevalence gradient with age across the other demographic strata. This suggests either a marked developmentally limited condition that tends to remit in the 3rd decade of life, or secular changes occurring in the prevalence of AUDs such that more recently born cohorts have higher prevalences. (It is also possible that high early mortality is partially responsible for the decline, but the size of the decline from the 18–29 group to the 30–44 group is far too large to make this a viable explanation for the most dramatic part of the curve.) Although there is some evidence to suggest that there are secular changes in the age of onset of AUDs, with recent cohorts showing an earlier onset than older cohorts (Reich, Cloninger, Van Eerdewegh, Rice, & Mullaney, 1988), existing data suggest that the age-related decline in prevalence is primarily a developmental phenomenon and is not attributable to secular trends in consumption patterns (Grant, 1997). Perhaps the most compelling data suggesting that AUDs are strongly developmentally graded come from prospective studies of heavy, episodic alcohol use and AUDs in young adulthood (e.g., Chen & Kandel, 1995; Schulenberg, O’Malley, Bachman, Wadsworth, & Johnston, 1996; Sher & Gotham, 1999).
Beyond revealing a mean decreasing trend in heavy drinking during the 20s, these same studies also indicate considerable variability in course. Schulenberg et al. (1996) identified several distinct trajectories of (so-called) binge drinking (defined here as five or more drinks in a row during the previous 2 weeks) over the age span of 18 to 24. None of these trajectories closely resembled the mean trajectory of relatively low levels of bingeing at age 18, slight increases from age 18 to age 19–20, stability, and then decreases beginning at age 21–22. These trajectories as were described as chronic (high levels of bingeing at all time points), decreased (high levels at age 18 that monotonically decreased to very low levels by age 23–24), increased (low levels at 18 monotonically increasing over time to very high levels by age 23–24), and fling (low levels at 18 and at 23–24 but moderately high levels during the middle years), with a rare trajectory that was characterized by infrequent bingeing at all time points.
These different trajectories were found to be distinguishable from each other on the basis of a range of etiologically relevant predictors such as gender, personality, drinking motivations, and the social context of drinking. Similarly, other data suggest that young adults show a decreasing likelihood of diagnosing with an AUD over time but with significant variation in course; some individuals tend to diagnose chronically, others show apparent remission after diagnosing early, and still others tending to increase in their likelihood of diagnosing over time (Sher & Gotham, 1999). Thus, although the mean trend of pathological alcohol involvement in young adulthood is toward maturing-out, so to speak, we also see the beginning stages of what might become a persistent lifecourse pattern in early adulthood. In addition, there is a small group of late starters who begin to show problematic alcohol involvement when their peers are recovering from such patterns. Thus, variability in course can be conceptualized as mixture of distinct trajectories.
An alternative perspective on variability in course is the state-trait model of psychopathology (Jackson et al., 2000). This model proposes that the tendency to diagnose over time is attributable to a stable trait that is indicated by the presence or absence of symptoms at multiple assessment occasions. From this perspective, the occurrence of an AUD at a particular point in time is a joint function of trait AUD and situational variables that tend to inhibit or facilitate the expression of the trait. Both trajectory and state-trait perspectives suggest that cross-sectional current diagnoses (based on recent symptom clustering) and retrospectively assessed, lifetime diagnoses (based on meeting of diagnostic criteria at some point in the individual’s life) fail to capture developmental aspects of AUDs and the related dimension of chronicity. Diagnostic approaches that attend more fully to course may prove to be important etiologically and clinically.
Comorbidity
As noted earlier, there is high comorbidity between AUDs and other Axis I and Axis II disorders. In the NCS (Kessler et al., 1997), lifetime alcohol dependence was robustly associated with higher rates of lifetime diagnoses of all anxiety, affective, drug, and antisocial behavior disorders surveyed; and this was true for both men and women. Consistent with data from the ECA (Helzer & Pryzbeck, 1988; Helzer et al., 1991), the disorders most strongly associated with alcohol dependence were mania, drug use disorder, and antisocial personality disorder. However, comorbidity with alcohol abuse was less consistent and those relations that were significant were less generalizable across gender.
Most NCS participants with an AUD had at least one of the disorders surveyed. Establishing whether the comorbidity with AUD was potentially causal, consequential, or attributable to some common etiological process is a major area of current interest. In order to characterize the nature of comorbidity better, many investigators have attempted to classify AUDs as either primary or secondary (Schuckit, 1985). This primary-secondary distinction is based upon the sequencing of onset of AUDs and of comorbid conditions. That is, when an AUD occurs prior to a comorbid condition it is considered primary; when it occurs subsequent to a comorbid condition it is considered secondary.
In the NCS, alcohol dependence was typically found to be secondary to other comorbid disorders (Kessler et al., 1997). In particular, alcohol dependence was found to be secondary to anxiety disorders (especially social phobia) and antisocial disorders (especially conduct disorder); and primary to drug use disorders and affective disorders. This is not surprising because, by definition, some disorders (e.g., conduct disorder) onset before midadolescence, and some disorders (e.g., depression) tend to have relatively late onset. Moreover, prior lifetime disorders tended to positively predict the onset of lifetime alcohol dependence across all disorders assessed. However, other prior lifetime disorders did not predict the onset of alcohol abuse consistently, and when they did predict, the patterns were difficult to interpret. For example, depression, mania, and drug dependence were found to be negatively associated with subsequent alcohol abuse in men and positively associated in women (Kendler et al., 1997). It seems likely that these seemingly anomalous results represent a statistical artifact of segregating out a mild form of AUD (abuse) from more severe forms (dependence). Alternatively, it might be useful to consider broadband diagnosis (abuse and dependence combined) and narrow-band dependence separately.
The retrospective analyses in both the NCS and ECA, although of interest, assume the accuracy of retrospective symptom reporting when trying to sequence disorders that may have been experienced decades earlier . . . a big assumption. Moreover, there can be co-occurrence between alcohol consumption and minor symptomatology prior to any formal symptom onset, and many symptoms (e.g., tolerance to alcohol, worry) can have insidious onsets and be difficult to date.
Unfortunately, there are few prospective studies of AUD comorbidity that would help unravel direction of causality. Those studies that do exist either cover early periods of development (e.g., Costello et al., 1999) during which participants have yet to pass through much of the period of risk for disorders, or begin later in development (e.g., Kushner, Sher, & Erickson, 1999) when extensive symptomatology is already in place. Costello et al.’s findings indicate that comorbidity processes can begin in childhood, further highlighting the difficulty of disentangling cause and effect using retrospective reports in adults.
To date, population-based epidemiology of comorbidity between AUDs and psychopathology has focused on the DSM Axis I disorders with the important exception of APD (and its childhood precursors), which was assessed in the ECA and NCS. Although the database for examining AUD/Axis II comorbidity is not well developed, existing studies suggest a strong relation between AUDs and both antisocial and borderline personality disorders (Sher et al., 1999), two disorders characterized by disinhibition. Other personality disorders associated with AUDs in multiple studies include borderline, histrionic, narcissistic, and avoidant. It is possible that much of the comorbidity among AUDs and Axis I comorbidity might be mediated via personality disorder or closely related traits.
Even well-conducted prospective studies beginning early in development are not capable of disentangling direction of effect between alcohol involvement and psychiatric symptomatology because it is possible that common third variables influence both alcohol involvement and comorbid conditions. For example, behavior-genetic investigations suggest that common genetic vulnerabilities are partially responsible for comorbidity between alcohol dependence and nicotine dependence (True et al., 1999), conduct disorder (Jang et al., 2000; Slutske et al., 1998), and to a lesser degree, anxiety disorders (Kendler et al., 1995; Merikangas et al., 1998) and depression (Prescott, Aggen, & Kendler, 2000). Identifying common vulnerability factors represents just a first step toward identifying the functional mechanisms transducing genetic influences. Differences in neurocognitive abilities and personality discussed earlier may represent heritable vulnerabilities mediating genetic influences on AUD and comorbid conditions.
Genetics
It has long been known that AUDs are strongly familial, that is, they tend to aggregate in the same families (e.g., Cotton, 1979). However, only in the past 20 years has a strong consensus developed that the cause of this familiality is genetic inheritance. This is because modern adoption and twin studies have clearly shown that much of the variation in risk for AUDs is attributable to genes rather than to the effect of living in a family environment that promotes AUD development. For example, adoption studies indicate that it is alcoholism in biological relatives and not alcoholism in the family of rearing that increases risk for offspring. Similarly, twin studies indicate higher concordance rates for AUDs in identical (monozygotic) twins than in fraternal (dizygotic) twins (see McGue, 1999b, for review; and note that there is also strong evidence for genetic effects on measures of alcohol intake [Heath, 1995a]). Nevertheless, there is some controversy in the genetic epidemiology literature concerning a number of issues, including whether there are distinct heritable subtypes or whether genetics play as important a role in women as in men (Hesselbrock, 1995; McGue, 1999b; Searles, 1988). Much of this inconsistency probably arises from the fact that many primary studies are underpowered and have variation in the operationalization of the phenotype studied, and that ascertainment biases surrounding use of clinical samples can lead to inaccurate estimates (Heath, 1995b; Searles). At present there appears to an emerging consensus that genetic factors are important in men and women, that multiple genes are responsible for the genetic effect, and that the nature of the genetic vulnerability remains to be discovered (McGue; National Institute on Alcohol Abuse and Alcoholism [NIAAA], 2000).
The search for identifying specific genes contributing to alcoholism risk is still at an early stage, but recent advances in molecular genetics now allow us to scan many genetic loci for possible association with alcoholism. Several chromosomal regions that appear to contain genes associated with alcoholism have been tentatively identified (Reich et al., 1998) and it seems likely that in the next several years, specific genes associated with alcoholism risk will be definitively identified and the mode of influence characterized.
One source of genetic influence on alcoholism risk appears to be mediated by individual differences in ethanol metabolism, at least in some populations. First, variation in two of the genes (alcohol dehydrogenase 2 and 3 [ADH2 and ADH3]) responsible for the enzymes that break down alcohol into its metabolite, acetaldehyde, appear to be related to alcoholism risk in Asian populations (Reich et al., 1998). One recent review concludes, “It can now be regarded as firmly established that . . . [genetic variants] encoding faster metabolizing forms of ADH2 and ADH3 reduce the risk that carriers of these [genetic variants] will develop alcoholism” (NIAAA, 2000, p. 176). Additionally, variation in one of the genes for aldehyde dehydrogenase (the enzyme that breaks down acetaldehyde, the toxic metabolite of alcohol, into acetic acid) is associated with alcoholism risk in Asians (e.g., Harada, Agarwal, Goedde, Tagaki, & Ishikawa, 1982). Those with a specific variant of the gene are at very low risk for alcoholism (i.e., they are protected). The relevance of this effect to those of European ancestry, however, is unclear because the prevalence of this genetic variation is very rare in Caucasians. Still, this finding indicates how specific genes could have an effect on alcoholism risk.
Much of the current research on the search for specific genes for alcoholism has focused on genes related to central nervous system functioning. As reviewed by Diamond and Gordon (1995), there are a number of plausible candidate genes related to different neurotransmitter mechanisms. These include genetic variation associated with the gammaaminobutyric acid (GABA)/benzodiazepine (BZ) receptor complex (important in anxiolysis), the N-methyl-D-aspartate (NMDA) receptor (an excitatory glutamate receptor known to be extremely sensitive to alcohol in physiological doses), calcium channels, cyclic adenosine monophosphate (cAMP), and G proteins. Additionally, there has been recent interest in genes regulating dopamine and serotonin transport (Lichtermann et al., 2000; Repo et al., 1999). However, to date, no genes related to brain function have been firmly linked to alcoholism risk. Previous reports that one genetic variant of the dopamine D2 receptor is associated with alcoholism have proven controversial and are not widely accepted (McGue, 1999; NIAAA, 2000). However, there is currently much interest in the possible association between the D4 receptor gene and a range of impulse-control disorders, including alcohol misuse (Zuckerman & Kuhlman, 2000). At this juncture, it seems likely that research currently underway will begin providing more definitive links between specific genes and alcohol dependence and point to specific etiological mechanisms.
Etiological Models
There are a number of theories of alcoholism etiology that have empirical support and that continue to be under active investigation. These various models are not mutually incompatible and there are likely to be multiple pathways into pathological alcohol involvement both between and within individuals. Four etiological models are highlighted here: (1) positive affect regulation, (2) negative affect regulation, (3) pharmacological vulnerability, and (4) deviance proneness. To varying degrees, each of these models is probably applicable not only to other forms of substance use disorder (e.g., cocaine dependence, opiate dependence) but, with the exception of the pharmacological vulnerability model, they are also likely applicable to PG and other impulse-control disorders.
Positive Affect Regulation
Most drinkers expect alcohol to be a positively transforming experience that directly produces pleasurable experiences (Goldman, Del Boca, & Darkes, 1999). Although expectations concerning the effects of alcohol begin early in childhood and prior to direct pharmacological experience (e.g., Noll, Zucker, & Greenberg, 1990), these expectations strengthen during adolescence with increasing alcohol experience (Smith, Goldman, Greenbaum, & Christiansen, 1995). Moreover, drinking for positive reinforcement or enhancement (e.g., drinking “to get high” and “because it makes you feel good”; Cooper, Russell, Skinner, & Windle, 1992) appears to be a primary dimension of drinking motives and is strongly associated both with positive expectancies for enhancement and with personality traits related to reward seeking (i.e., sensation seeking; Cooper, Frone, Russell, & Mudar, 1995) and appears to mediate these expectancy and personality effects on alcohol use.
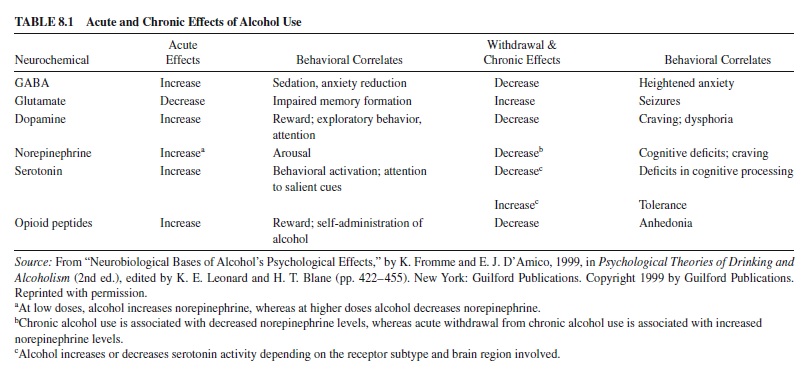
Presumably, these motivations for positive reinforcement from alcohol are based on alcohol’s neuropharmacological effects on the brain centers involved in basic reward mechanisms. For example, alcohol, like other drugs of abuse, has been shown to stimulate mesolimbic dopamine activity that is believed to be involved in basic reward mechanisms (Koob, 2000). In addition, alcohol has been shown to increase activity in brain opioid systems (Gianoulakis, 1996). As illustrated in Table 8.1, alcohol has effects on a range of neurotransmitter systems; several of these are related to positive reinforcement and others to negative reinforcement. Note that the chronic effect of ethanol is often in the opposite direction of the acute effect. For example, the profile of neuropharmacological activity and associated affects during withdrawal are in opposition to the corresponding profile of acute effects. This suggests that in early stages of alcohol involvement, reinforcement from use may predominate—but with chronic exposure, negative affect starts to develop, setting up a “spiraling addiction cycle” (Koob & Le Moal, 2001). That is, chronic use leads to dependence phenomena that provide further motivation for use.
Negative Affect Regulation
One of the most enduring etiological perspectives on alcoholism is that AUDs become established because of the relief of negative affect. There is certainly considerable evidence in support of this general model, which has sometimes been referred to as self-medication or the tension-reduction hypothesis (Cappell & Herman, 1972; Greeley & Oei, 1999; Sayette, 1999; Sher, 1987). As is true for expectancies for positive reinforcement, individuals hold strong expectations that alcohol reduces anxiety or stress (Fromme, Stroot, & Kaplan, 1993). They also report drinking to cope with negative affect (e.g., “to relax,” “to forget your worries,” “because it helps when you feel depressed or worried”) as a primary reason-for-drinking dimension (Cooper et al., 1992). These coping motivations are strongly related to both alcohol consumption and problems (see Sher, 1987) and mediate the effects of negative affect and tension-reduction expectancies on drinking outcomes (Cooper et al., 1995).
The animal literature indicates that alcohol can have powerful anxiolytic effects in certain paradigms. For example, alcohol has been shown to reliably decrease passive avoidance (i.e., it increases approach to reward in the presence of cues for punishment) in a way much like that of well-known anxiety-reducing compounds such as benzodiazepines and barbiturates (Cappell & Herman, 1972). Additionally, alcohol is known to affect the GABA/BZ receptor in many of the same ways that benzodiazepines do (see Table 8.1), although some paradigms for assessing emotions in humans suggest that the effect of alcohol is quite different than that of benzodiazepines (Stritzke, Patrick, & Lang, 1995).
The picture is further clouded because negative affective states, by themselves, have not been found to be strongly related to alcohol consumption or problems, and laboratorybased investigations of the effect of alcohol on negative affect have yielded confusing and contradictory evidence (Greeley & Oei, 1999; Sayette, 1999; Sher, 1987; Stritzke, Lang, & Patrick, 1996). Greeley and Oei (p. 41) concluded a recent review with the statement that “some individuals, for example, those who may be genetically predisposed to experience greater stress-buffering effects from alcohol, who hold certain beliefs about alcohol, will under certain circumstances consume alcohol for its stress-response-dampening effects.” Thus, contemporary research has demonstrated that alcohol can have negatively reinforcing properties and is consumed for these effects, but that the alcohol–negative affect relation is highly conditional upon a range of individualdifference, contextual, and response parameters.
Perhaps one of the most important formulations regarding the relation between alcohol effects and negative affect is that proposed by Steele and Josephs’ (1990) alcohol myopia model. According to this model, many of alcohol’s “prized and dangerous” effects are mediated by alcohol’s effects on attentional processes. Quite simply, alcohol narrows attentional capacity so that one can attend to only the most salient cues in the environment. Whether alcohol is found to be stress reducing can be moderated by the nature of the environmental context. If pleasant distractors are present and salient, these can take attentional precedence over less salient cues for punishment (or internal aversive thoughts) and serve to mitigate stress or anxiety. However, in the absence of cues to divert attention, alcohol can actually amplify negative affect by narrowing the attentional focus to only salient negative stimuli. That is, the affective consequences of intoxication are heavily moderated by contextual factors and, as discussed next, individual difference variables.
Pharmacological Vulnerability
The pharmacological vulnerability model (Sher, 1991) proposes that individuals differ in their responses to the acute or chronic effects of alcohol and that these individual differences are etiologically relevant. More than 100 years ago, Fere (1899) posited that “all subjects do not offer the same susceptibility to the actions of medicaments and poisons,” and noted that “Lasegue has specially insisted upon the differences of aptitude for intoxication.” The model itself incorporates several submodels that would appear to offer opposing predictions. For example, it can be hypothesized that some individuals are at risk for alcohol-related difficulties because they are especially sensitive to reinforcement (either positive or negative) and are therefore more likely to use alcohol because they get comparatively great effect from it. Alternatively, it can be hypothesized that some individuals are relatively insensitive to reinforcement and thus must consume relatively high amounts of alcohol to achieve a desired effect and thus expose themselves to high blood-alcohol levels, putting themselves at higher risk for alcohol-related organ damage and possibly physiological dependence.
Because of acquired tolerance, it is problematic to compare the alcohol sensitivities of alcohol-dependent individuals and controls. To get around this important methodological difficulty, a number of studies have compared nonalcoholics at high risk for later alcohol dependence with those at low risk. In these studies, risk status is predicated on family history of alcoholism. Reviews of the literature (Newlin & Thomson, 1990; Pollock, 1992) reveal a confusing pattern of findings, with some studies indicating that those at high risk show more pronounced alcohol effects (e.g., increased stress reduction or heart rate), whereas other studies show less pronounced alcohol effects (e.g., decreased body sway, decreased reports of intoxication). Newlin and Thomson (1990) reconciled these seeming discrepancies in noting that highrisk individuals show greater sensitivity when blood alcohol is rising and less sensitivity when blood alcohol is dropping. Because reward is more associated with rising blood alcohol and punishment with descending blood alcohol, they suggest that high-risk individuals are likely to experience both more reinforcement and less punishment than their low-risk counterparts, and that this pattern represents a very powerful form of pharmacological vulnerability.
Most data relevant to the pharmacological vulnerability model are based upon cross-sectional, high-risk versus lowrisk comparisons. Stronger evidence for the etiological relevance of individual differences in the pharmacological effect of alcohol involves the prospective prediction of later alcohol use disorders from baseline differences in alcohol sensitivity. Schuckit and Smith (1996) found, in an 8-year follow-up study of 450 men, that decreased alcohol sensitivity (especially with respect to subjective intoxication) was associated with the later development of AUDs. These findings are the strongest to date in implicating individual differences in alcohol sensitivity as a risk factor for alcoholism. However, because it is unethical to give alcohol-naive subjects alcohol in the laboratory, it is unclear to what extent these individual differences reflect constitutional differences in alcohol sensitivity or acquired tolerance. The mechanisms underlying variability in sensitivity remain unclear, but it does not appear to be due to differences in ethanol metabolism.
Deviance Proneness
A final model to consider concerns what has been termed deviance proneness (Sher, 1991). The key notion here is that excessive alcohol involvement comes about not so much because of attempts at regulating affective states or because of any particular vulnerability to alcohol as a drug but because alcohol use is part of a more general, deviant pattern that has its roots in childhood and is attributable to deficient socialization. In a probing review of the early development of alcohol problems, Zucker et al. (1995; see also Zucker & Gomberg, 1986) note consistency across extant longitudinal studies of alcoholism that begin in childhood. These studies highlight a number of commonalities, including a history of childhood antisocial behavior problems, childhood achievement problems, poorer childhood interpersonal relations, heightened activity in childhood, less parent-child contact, and inadequate parenting. Several explanatory models have been put forth to explain the relation between these correlates and early alcohol use and other problem behaviors. Perhaps the best known of these is problem-behavior theory (Donovan & Jessor, 1985; Jessor & Jessor, 1977), which posits that a range of personality, family, peer, and other environmental variables causally relate to involvement in a range of deviant behaviors including early alcohol use, illicit drug use, precocious sexual activity, and school failure. From this perspective alcohol involvement is only one indicator of a broader factor of general deviance, although the hypothesized causal structure among problem behaviors and their mediators differs (Kaplan, 1975; Oetting & Beauvais, 1986; Windle & Davies, 1999).
Although this model emphasizes deficient socialization as evidenced by decreased attachments to family, school, and religious institutions and increased involvement with deviant peers, personality and temperamental variables are often viewed as distal influences on these social, developmental processes (Petraitis, Flay, & Miller, 1995). Consequently, genetic influences on personality are probably very relevant to these ostensibly social processes. Moreover, the same personality traits that put into place these problematic behavior trajectories (e.g., impulsivity) can also have proximal effects on alcohol use in the form of risky decisions about alcohol use and other behaviors (Sher et al., 1999).
Drug Use Disorders
A recent report commissioned by the Robert Wood Johnson Foundation chronicles the consequences of drug use in the United States (Horgan et al., 2001). The number of deaths directly attributable to drug use has more than doubled over the last two decades, and is approaching the number of deaths directly attributable to alcohol. Most of these deaths directly attributable to drugs were associated with overdoses of heroin or cocaine, especially a lethal combination of heroin or cocaine with alcohol or other drugs. There are also many deaths that are indirectly associated with drug use, such as deaths from suicide, hepatitis, and tuberculosis, and from AIDS among injecting drug users. Drug use is also associated with motor vehicle crashes, other types of accidents, and crime (Horgan, Skwara, & Strickler, 2001).
Despite all of the negative publicity, heroin, especially if it is not adulterated, does not cause as much physical harm as many of the more common drugs of abuse. Much of the medical harm associated with heroin use is due to poor nutrition, the use of adulterated heroin, the sharing of needles, and other lifestyle factors. Inhalant use disorders, compared to the other drug use disorders, are the most likely to cause medical harm to those affected. Inhalants are especially toxic to the nervous system, but can also cause damage to the heart, lungs, kidney, liver, blood, and other systems (Kuhn, Swartzwalder, & Wilson, 1998).
History of Drug Use Disorders in the United States
In this section, we cover drugs that are illegal or, legal when prescribed by a health professional, are used for nonmedical purposes. The problem of drug abuse in the United States is inextricably linked with the history of the legislation that has led to the regulation and eventual criminalization of these drugs. Perhaps the single piece of legislation that most reduced drug use disorders in the United States was also the first law dealing with the regulation of drugs: the Food and Drug Act of 1906 (Bonnie & Whitebread, 1974), which required manufacturers to provide lists of the ingredients in their products. Prior to this, many Americans were unwittingly becoming addicted to opiates and cocaine simply by using products readily available at their local stores or from traveling salesmen.
In response to the mounting problem of opiate and cocaine addiction in the early twentieth century, the Harrison Tax Act was passed in 1914 and represented the first attempt of the U.S. government to control drug addiction through criminal sanctions. Individuals who were found in possession of heroin or cocaine were arrested for tax evasion, rather than for criminal possession of a drug (Bonnie & Whitebread, 1974). Soon after, several Supreme Court rulings made it illegal for doctors to prescribe drugs to those who were addicted, which meant that the only means for acquiring drugs were illegal (King, 1972) and many addicts were imprisoned. In response to the growing problem of overcrowding in federal prisons, Congress authorized the U.S. Public Health Service to establish hospitals (one opening in Lexington, Kentucky, in 1935, and the other in Ft. Worth, Texas, in 1938) where addicted individuals convicted in federal courts could serve their terms (King, 1972).
In 1915, Utah became the first state to pass a criminal law against the use of marijuana, and many other states soon followed. In 1937, the United States passed the Marijuana Tax Act, which heralded the beginning of the U.S. national prohibition of marijuana. Over the ensuing years, the U.S. government and individual states dealt with the problem of drug addiction by imposing increasingly strict penalties for drug possession that were often harsher than penalties for violent crimes like rape (Bonnie & Whitebread, 1974). In 1970, in order to bring some order to a complex array of antidrug laws, the U.S. Comprehensive Drug Abuse Prevention and Control Act repealed, replaced, or updated all previous antidrug laws (King, 1972). This act classified the drugs of abuse into schedules, according to their medical utility and abuse potential (Goode, 1999), and linked penalties for distribution and possession to these schedules. The Schedule I drugs (the most severe category) included heroin, LSD, hallucinogens, and marijuana; these drugs were considered to have no acceptable medical use and high potential for abuse. (Since passage of this act, many states have decriminalized the possession and use of small amounts of marijuana.) As new drugs of abuse enter the marketplace (e.g., 3, 4-Methylenedioxymethamphetamine [MDMA, or Ecstasy]), they are placed into this schedule. Despite decades of criminalization of drug use and prevention, the drug problem is probably as severe now as it was prior to regulation and prohibition.
Another perspective on the history of drug abuse in the United States comes from changes in drug-use disorder classifications over successive revisions of theDSM.The drug use disorders have been recognized as a mental illness since the DSM-I (APA, 1952), but as with alcohol use disorder, they were considered a subtype of sociopathy until the DSM-III (APA, 1980), when a new substance use disorder section was added. The DSM-III described drug use disorders associated with seven different substances (in addition to alcohol and tobacco): sedative-hypnotic-anxiolytics, opiates, amphetamines, cannabis, cocaine, phencyclidine (PCP), and hallucinogens. The DSM-III recognized drug abuse for all seven substances, but drug dependence was possible for only four of the seven because there was no evidence at the time that tolerance or withdrawal were associated with cocaine, PCP, or the hallucinogens (APA, 1980). It was not until the DSM-III-R in 1987 that cocaine withdrawal and cocaine dependence were officially recognized (APA, 1987). Although tolerance is probably associated with all of the drugs considered in the DSM, problems in assessment (discussed with respect to alcohol earlier in this research paper), variability in the potency of street drugs due to their unregulated nature and potency differences among drugs within a class can make it difficult to establish.
In the DSM-III-R, inhalants were added and the diagnostic criteria for the substance use disorders were standardized to be the same across substances, and both abuse and dependence were recognized for all eight drug classes listed. In the DSM-IV, a drug dependence was further specified as being with or without physiological dependence for all substances except hallucinogens and PCP, for which the existence of a withdrawal syndrome is still somewhat uncertain (APA, 2000).
Epidemiology
In the NLAES study, the combined lifetime prevalence of drug use disorders according to DSM-IV criteria was 6.1%. (It is worth noting that the ECAstudy provided an estimate of [DSM-III] lifetime drug use disorder prevalence of 6.2%; Anthony & Helzer, 1991.) In NLAES, the highest prevalences were for cannabis use disorder (4.6%); a composite category of prescription drug use disorder incorporating sedatives, tranquilizers, opiates, and amphetamines (2.0%); cocaine use disorder (1.7%); and amphetamine use disorder (1.5%). The lifetime prevalences of disorder for the remaining drug classes (sedatives, tranquilizers, and hallucinogens) were each less than 1.0% each (Grant & Pickering, 1996). Because of the relatively low prevalences of specific drug use disorders and the substantial comorbidity among them (discussed shortly), most of the epidemiologic research (other than the behavioral genetic studies, again, discussed shortly) focuses on composite diagnoses of drug use disorder.
Although the NCS provided higher lifetime (n.b., DSMIII-R) prevalence estimates than did NLAES for drug dependence (7.5%) and abuse (4.4%; Kessler et al., 1994), there was consistency with NLAES in the relative prevalence of specific drug dependence, with cannabis being the most prevalent at more than 4.0%, following by cocaine (2.7%) and amphetamines (1.7%). The remaining lifetime prevalences of dependence for the remaining drug classes were each less than 1.2% (Anthony, Warner, & Kessler, 1994). Because drug use disorders tend to be developmentally limited, past-year prevalence estimates are much lower than lifetime estimates. For example, the past-year prevalence of any drug use disorder in the NCS study was 1.8% (Warner, Kessler, Hughes, Anthony, & Nelson, 1995) as compared to a lifetime prevalence of 11.9%. In general, lifetime drug use disorders are higher among young white men with fewer years of education and lower incomes, and residing in urban areas (Anthony & Helzer, 1991;Anthony et al.).
Comorbidity
In the ECA study (Anthony & Helzer, 1991) individuals with a DSM-III lifetime drug use disorder were 2 to 11 times more likely to have a comorbid psychiatric disorder than those without a history of drug use disorder, with the largest increases in relative risk for drug use disorder among those with mania and APD, followed by schizophrenia, depression, alcohol use disorder, and the anxiety disorders. The patterns of comorbidity were similar for men and women, except that the increased rates of drug use disorders among women with APD and alcohol use disorders were relatively much higher than among men.
Large national samples have conclusively demonstrated high comorbidity among specific drug use disorders and between alcohol use disorders and drug use disorders. For example, in NLAES (Grant & Pickering, 1996), each of the specific drug use disorders was strongly associated with alcohol use disorder, with odds ratios ranging from 13 to 27. Lyons et al. (1998) present the associations of the specific lifetime DSM-III-R drug use disorders with each other, using a large national community-based sample of middle-aged men. Again, the various drug use disorders were all strongly associated with each other, with odds ratios ranging from 12 (between opiate and cannabis use disorders) to 68 (between amphetamine and a combined category including hallucinogen and PCP use disorders). In sum, there is substantial comorbidity within the drug use disorder category, between drug use disorders and alcohol use disorders, and between drug use disorders and other psychiatric disorders. Polysubstance abuse–dependence and comorbidity appear to be the rule, rather than the exception.
Genetics
There has been much less published research on the genetics of drug use and drug use disorders compared to alcoholism, although it is presumed that the genetic risk for drug use disorders will overlap with the genetic risk factors for alcohol use disorders. Because there have been increases in the lifetime prevalence of drug use and drug use disorders in more recently born cohorts, the interpretation of studies that examine intergenerational patterns (e.g., family studies and adoption studies) is problematic because of secular changes in drug exposure and availability. Consequently, within-generation behavioral genetic studies of drug use disorders are the most straightforward to interpret.
Two recent large community-based twin studies of drug use disorders provide valuable within-generation information on the familial transmission of a composite diagnosis of drug use disorder and the specific drug use disorders. Tsuang et al. (1996) conducted a study of DSM-III-R drug use disorders in a large sample of twins from the Vietnam Era Twin Registry, a national sample of male twin pairs (born between 1939 and 1957) in which both men served in the U.S. military during the Vietnam era. Kendler and colleagues (Kendler & Prescott, 1998a, 1998b; Kendler, Karkowski, & Prescott, 1999; Kendler, Karkowski, Neale, & Prescott, 2000) conducted a population-based study of DSM-IV drug use disorders among male (born between about 1936 and 1978) and female (born between about 1933 and 1975) adult twin pairs born in the state of Virginia. With only a few exceptions, the results of these two studies support the existence of substantial genetic influences and very modest family environmental influences on the risk for drug use disorders. Heritability estimates for different classes of drugs ranged from .25 to .76 among men and from .72 to .79 among women for more broadly-defined drug use disorder (drug abuse or dependence), and from .58 to .97 for more narrowly-defined drug use disorder (drug dependence) amongs men (results for drug dependence among women are not available; Kendler & Prescott, 1998a, 1998b; Kendler, Karkowski, & Prescott, 1999; Kendler et al., 2000;Tsuang et al., 1996). In contrast, estimates of the proportion of variation in risk due to family environmental influences ranged from 0 to .32 among men and stood consistently at 0 among women (Kendler & Prescott, 1998a, 1998b; Kendler, Karkowski, & Prescott, 1999; Kendler et al., 2000; Tsuang et al., 1996).
In a follow-up multivariate analysis, Tsuang et al. (1998) examined the extent to which the familial risk for each specific drug use disorder was shared versus the extent to which it was specific to the drug. They found that most of the familial risk for the different drug use disorders could be explained by common genetic and environmental factors, with significant specific genetic influences on the risk for opiate use disorder and specific family environmental influences on the risk for cannabis use disorder. Kendler, Karkowski, Corey, et al. (1999) examined the extent to which genetic variation in risk for drug use disorder could be explained by genetic factors associated with the initiation of substance use, and found that, on average, about half of the genetic variation in drug use disorder was associated with genetic effects on substance use initiation. These findings are extremely important in that they indicate that different etiological processes are involved in substance use experimentation (a necessary precondition for drug use disorders) and the development of drug abuse or dependence once drug use is initiated. Future behavioral genetic studies of drug use disorders focusing on the influence of genetic and environmental factors across the various stages in the disorders’ development, starting with initiation and culminating with the final outcome of disorder, will be extremely valuable (Tsuang et al., 1999) but also difficult given the large sample sizes and the complexity of models that will be required.
Neurobiological Substrates of Drug Effects
Different drugs of abuse vary in their spectrum of effects on neurotransmitter systems, specific brain regions, and associated motivational systems. However, there are some important, shared commonalities among these pharmacologically distinct agents. As noted in Table 8.2, all commonly abused psychoactive drugs involve dopamine systems and, to a slightly lesser extent, the opioid peptide system (which is intimately linked to the dopamine system; e.g., Koob & Le Moal, 2001). One influential theory of addiction (Wise & Bozarth, 1987) posits that “all addictive drugs have psychomotor stimulant properties and that the biological mechanism of the psychomotor stimulant properties is the same as, or has common elements with, the biological mechanism of the reinforcing effects of these drugs” (p. 482). That is, there is a common reward mechanism underlying the effects of different addictive drugs. This is not to say, however, that different drugs of abuse exert their addictive properties through only one site of action. Indeed, different drugs of abuse show affinities to distinct classes of receptors, and their effects on dopamine and opioid systems may be indirect. As noted by Koob and Le Moal (2001, p. 103), “drugs may enter into this neurocircuitry at different points and via different molecular/cellular mechanisms.”
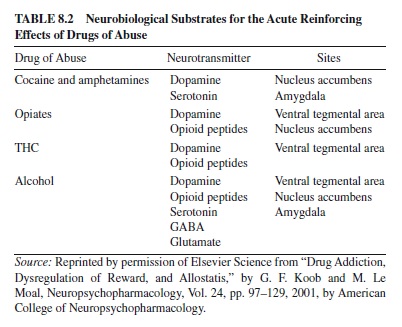
From a neurobiological perspective, vulnerability to drug abuse can come about either because of individual differences in the initial reinforcing properties of a drug or because of individual differences in compensatory mechanisms (e.g., initial opponent processes or allostatic progression) discussed earlier. Unfortunately, longitudinal research in humans that attempts to chart neurobiological changes associated with differing patterns or trajectories of drug involvement have yet to be conducted.
Etiological Models
Etiological theories of drug use disorders tend to parallel those described under alcohol use disorders (i.e., positive and negative affect regulation, pharmacological vulnerability, and deviant socialization). However, a major distinction between alcohol use and illicit drug use is the fact that alcohol use is legal for adults, whereas use of illicit drugs, by definition, is not. Consequently, use of alcohol is more readily integrated into mainstream culture, and initial exposure, even for minors, is inherently less of a deviant social behavior. Thus, models of deviant socialization are particularly relevant to drug use disorders, especially as they relate to experimental substance use.
Petraitis et al. (1995) recently reviewed 14 models of experimental substance use that have received empirical evaluation in the research literature. Based on their synthesis of these theories, which varied widely with respect to focus and constructs employed, they developed a matrix of influences on experimental use. This matrix is defined by types of influence (i.e., social-interpersonal, cultural-attitudinal, and intrapersonal) and level of influence (i.e., ultimate, distal, and proximal), yielding nine cells of this matrix. For example, ultimate influences include parental divorce or separation (social-interpersonal), local crime and unemployment (cultural-attitudinal), and temperament or personality (intrapersonal). Distal influences include attachment to parents and peers (social-interpersonal); weak commitment to conventional values, school, and religion (cultural-attitudinal); and psychological distress (intrapersonal). Proximal influences include perceived norms for use (social-interpersonal), expected utilities of substance use (cultural-attitudinal), and refusal skills and intentions to use substances (intrapersonal). Petraitis et al. argue that a comprehensive theory of experimental substance use needs to address both the level and the type of influence in order to be complete. This approach appears to be a useful first step toward organizing constructs involved in the literature and illustrates why some types of models (e.g., models that focuses more on proximal as opposed to distal or ultimate processes) should predict initiation of use better than others. However, it is more of a framework than a theory in that it is relatively agnostic toward identifying key causal mechanisms.
Pathological Gambling
It is a matter of continuing controversy whether the overall costs to society of PG, including costs associated with indebtedness, unemployment, and loss in productivity; thefts and criminal justice system costs; welfare costs; and treatment costs for individuals with PG and their spouses are outweighed by the economic benefits to society of gambling (National Research Council, 1999). What is not controversial is that PG has considerable negative economic and psychological effects on individuals and families. Although there is little direct evidence supporting a causal link, there seems to be little disagreement that PG can precipitate the types of stressful life events that are associated with an increased risk of depression and suicide (Blaszczynski & Farrell, 1998). Perhaps it is no coincidence that Las Vegas has the highest suicide rate of any city in the United States (Phillips, Welty, & Smith, 1997).
History of Pathological Gambling in the United States
The legality and availability of gambling have changed dramatically over the past two decades, and currently most adults have engaged in some form of gambling (86%; Gerstein et al., 1999). Prior to the late 1980s, the only legal gambling options in the United States were gambling in Nevada and Atlantic City, and state-run lotteries. In the late 1980s, gambling on Native American land or on riverboat casinos was legalized, and in the mid-1990s Internet-gambling Web sites were introduced. By 1999, gambling in some form was legal in 48 states; 21 states had casinos, 37 states had a lottery, and there were more than 650 Internet gambling sites worldwide. The number of Internet gambling sites has since doubled. The prevalences of gambling participation (Gerstein et al.), and of PG and problem gambling (Shaffer, Hall, & Bilt, 1999), have increased along with the growth of gambling venues.
Pathological gambling was introduced into the official diagnostic nomenclature with the publication of the ninth edition of the International Classification of Diseases in 1977, followed by its inclusion into the DSM-III in 1980 (APA, 1980). However, the concept of compulsive gambling was widely accepted prior to its inclusion in the DSM-III: Gambling problems were recognized by Freud (1928/1961) and other psychoanalysts (e.g., Bergler, 1936, 1943, 1957) in the first half of the twentieth century, the self-help community of Gamblers Anonymous was founded in 1957, and the first specialty treatment program for gambling problems was created in 1968 (Petry & Armentano, 1999).
Pathological gambling is classified as an impulse-control disorder along with kleptomania, trichotillomania, pyromania, and intermittent explosive disorder. Although the diagnostic criteria for PG have changed over the subsequent revisions of the DSM, the essential feature remains the same: persistent and recurrent maladaptive gambling behavior that disrupts personal, family, or vocational pursuits (APA, 1994). With the revision of the DSM-III (DSM-III-R;APA, 1987) the diagnostic criteria for PG were modified to be parallel to the criteria for the substance use disorders, and included concepts of preoccupation, loss of control, tolerance, and withdrawal. In support of this conceptualization, surveys of individuals in treatment for PG have found that 45% to 89% felt that they needed to gamble progressively more to achieve the desired excitement (Bradford, Geller, Lesieur, Rosenthal, & Wise, 1996; Griffiths, 1995), and 33% to 87% felt irritable or restless after stopping or cutting back on their gambling (Bergh & Kuehlhorn, 1994; Bradford et al.; Wray & Dickerson, 1981). A distinctive feature of PG not shared with the substance use disorders is chasing—that is, returning to a gambling activity in an attempt to win back losses. Chasing losses is considered by some experts to be a pathognomonic symptom of PG, and represents the mechanism by which individuals who gamble can become ensnared in the downward spiral of problems (Lesieur, 1984).
The Nature of Gambling Activities
The variety of gambling activities available differ along several dimensions that may make them more or less likely to lead to PG or problem gambling (i.e., problematic gambling that does not reach threshold for a diagnosis of PG). By definition, gambling involves a certain amount of chance, but different activities vary in the amount of chance versus skill involved. The outcome of a bet can be decided in a matter of seconds to as long as several weeks, and either the winnings can either be immediately reinvested or there may be a time interval before the next bet can be made. For some gambling activities the bet-to-win ratio is extremely large, and for others the odds are nearly even. Finally, some activities are readily available and convenient whereas others are relatively less convenient; some gambling activities are solitary, whereas others require interacting with other people. The two dimensions that have been most consistently linked with PG and problem gambling are the chance-skill continuum and the continuous-discontinuous continuum. It has been suggested that games that require some skill (or perceived skill) and are more continuous, or high action, are more likely to be related to the development of problems (Walker, 1992). However, the strongest and most consistent predictor of PG or problem gambling is not necessarily the type of activity, but rather the number of gambling activities (Sproston, Erens, & Orford, 2000; Volberg & Banks, 1994).
It is possible that different gambling activities represent indicators of an underlying continuum of gambling involvement, with some activities being very common and indicative of lower levels on this continuum and other activities being less common and indicative of higher levels. Evidence consistent with this comes from a nationally representative survey of adolescents and adults in Great Britain (Sproston et al., 2000). Respondents were divided into groups according to whether they had participated in one, two, three, four, five, or six or more different gambling activities in the past year. With each additional activity, all of the activities of the less involved groups were endorsed by the majority of the individuals in the more involved groups. That is, gambling activities appeared to conform to a Guttman scale progressing from participation in the national lottery, to scratchcards, to fruit (slot) machines, to private betting with friends, to horse races, and to dog races. Thus, in Great Britain, lottery playing is much less strongly associated with pathological and problem gambling than is betting on dog races.
Epidemiology
A recent meta-analysis of 119 North American PG prevalence studies conducted between 1977 and 1997 estimated the lifetime prevalence of diagnosable PG among adults at 1.6%, and the lifetime prevalence of subclinical PG, or problem gambling (i.e., endorsing at least one symptom of PG but not meeting the full criteria for a diagnosis; Shaffer et al., 1999) at 3.9%. The estimated lifetime prevalences of PG and problem gambling in a recent, nationally representative survey of 2,417 adults in the United States were 0.8% and 9.2%, respectively (Gerstein et al., 1999). Thus, between 5 and 10% of the U.S. population will experience problems with gambling at some point in their lives.
These gambling problems are unevenly distributed throughout the population. The prevalence of PG is higher (a) among men than women, (b) among younger than older individuals, (c) among individuals with fewer years of formal education than those with more education, (d) among individuals with lower income levels than the more advantaged, and (e) among indigenous peoples than other racial and ethnic groups (Volberg & Abbott, 1997; Welte, Barnes, Wieczorek, Tidwell, & Parker, 2000). The prevalence of PG is also higher among Blacks (Gerstein et al., 1999; Welte et al.) and Asian Americans (Welte et al.). It is unclear the extent to which these demographic correlates reflect differences in access to gambling venues, differences in the propensity to gamble, or differences in the propensity to fall prey to gambling problems given participation in gambling activities.
Comparisons of the prevalences of PG and problem gambling across geographic regions that differ in the availability of gambling suggest that greater access to regulated forms of gambling may be responsible for higher rates of PG and problem gambling. For example, comparisons across the eight states and territories within Australia yielded a correlation of about 0.65 between the per capita number of electronic gaming machines in a state or territory and the past-year prevalence of PG or problem gambling (Productivity Commission, 1999). Because of the historical and geographic variation in the accessibility of legal forms of gambling, it is important to know when and where a particular study took place because the prevalence, correlates, and causes of PG may vary with these different environmental contexts.
Genetics
Numerous studies have demonstrated that gambling involvement and problems run in families (e.g., Gambino, Fitzgerald, Shaffer, & Renner, 1993), although all of the extant studies relied on the family history method rather than on directly interviewing family members of index cases. Many experts attribute the familial transmission of gambling and PG to social-modeling influences (e.g., Gupta & Derevensky, 1997), but this conclusion is based upon the observation of parent-offspring transmission in nuclear families, which could be due to genetic as well as environmental factors. The role of a possible underlying biological diathesis in the development of PG has not been ignored by researchers; in fact, the search for putative indicators of biological vulnerability for PG (Blanco et al., 1996; Carrasco, Saiz-Ruiz, Hollander, Cesar, & Lopez-Ibor, 1994; Roy et al., 1988) and specific susceptibility genes associated with PG (Comings et al., 1996) actually preceded the behavioral genetic research documenting the importance of genetic influences on the risk for PG. Thus far, molecular genetic research on PG has focused on genes that have been claimed to show promise for explaining genetic variation associated with alcohol dependence (the dopamine D2 receptor [Comings et al.] and serotonin transporter [de Castro, Ibanez, Saiz-Ruiz, & Fernandez, 1999] genes) and the personality trait of novelty seeking (the dopamine D4 receptor gene [Comings et al.]).
Compared to research on substance use disorders, the behavioral genetic literature on PG is scant, consisting of a single study. In the Vietnam Era Twin Registry, the lifetime rates of DSM-III-R PG were significantly elevated among the monozygotic (23%) and dizygotic (10%) co-twins of men with PG, compared to the lifetime prevalence in the full sample (1.4%; Eisen et al., 1998). It was not possible to discern whether this familial similarity for PG was due to genetic or environmental factors because of the low base rate of PG, but it was possible to estimate that the total percentage of variation in the risk for PG that was accounted for by all familial factors (genetic and environmental) was 62%. In a follow-up combined (and more powerful) analysis of PG and alcohol dependence, Slutske et al. (2000) found that 64% of the variation in the risk for PG could be accounted for by genetic factors, with the remaining variation accounted for by individual-specific environmental factors or errors of measurement. Familial environmental factors did not significantly contribute to variation in PG, although these factors may still be important either in mediating genetic effects or in their interaction with an existing genetic predisposition. The results of this study suggest that PG is as heritable as alcohol dependence, and that genetic factors, rather than social modeling, predominantly explain the familial transmission of PG. However, it is unclear the extent to which this single study of PG among middle-aged men conducted in the early 1990s can be generalized to women, adolescents, or certain minority groups, or to the current gambling milieu.
Comorbidity
Reviews of the (primarily) clinical literature suggest that the rates of substance use disorders (Crockford & el-Guebaly, 1998; Spunt, Dupont, Lesieur, Liberty, & Hunt, 1998), mood and anxiety disorders (Crockford & el-Guebaly), and antisocial behavior disorders (Slutske et al., 2001) are significantly elevated in treatment-seeking individuals with PG compared to those without PG. However, comparisons of individuals with PG in treatment and in the community suggest that treatment samples are not representative of individuals with PG in the community (Volberg & Steadman, 1988) because less than 2% of individuals with PG report having ever received PG treatment (Wallisch, 1996). Six studies have reported the rates of comorbid psychopathology among individuals with PG recruited from the community, and only three of these studies were based upon randomly selected representative samples that included appropriate controls (Bland, Newman, Orn, & Stebelsky, 1993; Cunningham-Williams, Cottler, Compton, & Spitznagel, 1998; Smart & Ferris, 1996).
Although PG was not included in the ECA or NCS studies, it was included in one of the particular ECA sites. Symptoms of PG were assessed in the St. Louis ECAstudy in 1981, prior to the introduction of legal gambling to the St. Louis area (Cunningham-Williams et al., 1998). In the St. Louis ECA sample, problem gambling was significantly associated with alcohol abuse or dependence and nicotine dependence, but not with other substance use disorders. Problem gambling was also significantly associated with major depression and phobias, but not with panic disorder, generalized anxiety disorder, or obsessive-compulsive disorder. The strongest association obtained was between problem gambling and APD. Problem gambling was also significantly associated with schizophrenia and somatization disorder (Cunningham-Williams et al.). These findings are consistent with other community-based studies in finding elevated rates of alcohol use disorders (Black & Moyer, 1998; Bland et al., 1993; Slutske et al., 2000; Smart & Ferris, 1996) andAPD (Black & Moyer; Bland et al.; Cunningham-Williams, Cottler, Compton, Spitznagel, & Ben-Abdallah, 2000; Slutske et al., 2001) among individuals with PG or problem gambling. These are the most robust findings in the PG comorbidity literature. Results on the associations of PG with the mood and anxiety disorders are more mixed, and most studies since the St. Louis ECA study have found increased prevalences of other substance use disorders among individuals with PG or problem gambling (Black & Moyer; Bland et al.). There are also studies suggesting that the prevalences of DSM personality disorders from all three clusters (i.e., odd-eccentric, dramatic-erratic, and anxious-inhibited) are elevated among individuals with PG (Black & Moyer; Blaszczynski & Steel, 1998).
The causes of comorbidity of PG with other substance use and psychiatric disorders have not been extensively studied and there is little in the way of prospective longitudinal research tracking the temporal course of PG and comorbid conditions. Retrospective studies suggest that substance use disorders tend to precede PG in the majority of cases (Cunningham-Williams et al., 1998, 2000; Ramirez, McCormick, Russo, & Taylor, 1983). These findings are difficult to interpret because the apparent temporal sequencing may merely reflect age-related differences in the availability of gambling activities, disposable income, and psychoactive substances.
It is clear that alcohol and drug use often accompany gambling (e.g., Giacopassi, Stitt, & Vandiver, 1998), and concurrent gambling and substance use may be especially common among individuals with gambling problems (Spunt et al., 1998; Wallisch, 1996). Thus, the situational covariation of gambling and substance use may increase the likelihood of developing, maintaining, or exacerbating both gamblingrelated and substance use–related problems.
Alcohol intoxication may alter the perception of the likelihood of negative consequences of risky activities (Fromme, Katz, & D’Amico, 1997), or may lead to more general impairments in cognition and judgment that may result in poor decisions during gambling that may increase the likelihood of an adverse outcome. Several experimental studies have demonstrated that subjects are more willing to gamble or gamble more when under the influence of a moderate dose of alcohol than when given a placebo (Kyngdon & Dickerson, 1999; Sjoberg, 1969; Steele, 1986), although there are also studies that fail to find a causal link between alcohol use and willingness to gamble in a laboratory task (see Breslin, Sobell, Cappell, Vakili, & Poulos, 1999, for a review). To our knowledge, there are no experimental investigations testing the reverse-causal hypothesis that gambling may lead to an increased use of alcohol or other drugs, although the possibility is quite plausible.
Behavior genetic studies suggest that some proportion of comorbid substance use disorder and PG is due to a shared diathesis. Rates of alcohol-related problems among parents and other family members of individuals with PG appear to be higher than in the general population (Dell, Ruzicka, & Palisi, 1981; Lesieur, Blume, & Zappa, 1986; Lesieur et al., 1991; Linden, Pope, & Jonas, 1986; Ramirez et al., 1983; Roy et al., 1988). In the Vietnam Era Twin Study, there was significant familial cross-transmission of PG and alcohol dependence, suggesting a common vulnerability. Most of the genetic and environmental variation in the risk for PG was unique and not shared with alcohol dependence, but a significant fraction of genetic (12–20%) and individual-specific environmental (3–8%) vulnerability for PG was shared with alcohol dependence. It is important to recognize that these estimates subsume all possible reasons for the association between the genetic risk for PG and alcohol dependence, including pleiotropy (i.e., the presence of a genetic locus that jointly increases the risk for both PG and alcohol dependence) and indirect causal chains such as gene(s) Æ PG Æ AD and gene(s) Æ AD Æ PG.
There are two main lines of research linking PG and the antisocial disorders—the literature on delinquent youth suggesting a strong association of delinquency with PG and problem gambling, and the literature on adults with PG suggesting that PG can be a cause of criminal activities. Among youth, antisocial behavior appears to be the best concurrent predictor of gambling frequency in both boys and girls (Stinchfield, 2000). Although adults with PG are more likely to retrospectively report a history of childhood conduct disorder than adults without PG (Slutske et al., 2001), and the retrospectively reported age of onset of comorbid APD typically predates the onset of PG (Cunningham-Williams et al., 2000), the few attempts to predict gambling or problem gambling among adolescents or young adults from earlier involvement in delinquent activities have yielded mostly negative findings (Vitaro, Ladouceur, & Bujold, 1996; Winters, Stinchfield, Botzet, & Anderson, 2001). Thus, a causal influence of antisocial behavior on later PG has not been established.
Conclusions about the causal influence of PG on crime are based upon (a) retrospectively reported ages of onset of PG and crime, (b) the types of criminal activities that are involved, and (c) judgments of individuals with PG concerning the extent to which their crimes were gambling related (see Blaszczynski & Silove, 1996). Although there are no prospective studies or any experimental evidence supporting a causal link, the evidence is still quite convincing that crime is in some cases a consequence of PG. In fact, gambling-related crime constituted two of the seven diagnostic criteria for PG in the DSM-III: “arrest for forgery, fraud, embezzlement, or income tax evasion due to attempts to obtain money,” and “borrowing of money from illegal sources (loan sharks)” (APA, 1980, p. 293). One of these criteria has been modified and reinstated in the criteria for PG in DSM-IV: “has committed illegal acts such as forgery, fraud, theft, or embezzlement to finance gambling” (APA, 1994, p. 618). In the DSM-IV field trials, this item was less sensitive than the other symptoms of PG (endorsed by 65% of individuals with a PG diagnosis compared to 78–94% for other symptoms) but was more specific (endorsed by none of the participants without a PG diagnosis; Bradford et al., 1996). Involvement in illegal activities to finance gambling appears to be a more psychometrically difficult indicator of PG, suggesting that only individuals with more severe problems and who have hit bottom, so to speak, will resort to such behaviors.
A genetic basis for comorbidity between antisociality and PG is supported by the finding of significant familial crosstransmission of PG with childhood conduct disorder, adult antisocial behavior (the adult criterion for APD), and APD in the Vietnam Era Twin Study (Slutske et al., 2001). As with alcohol dependence, there was a significant fraction of genetic (26%) and individual-specific environmental (7%) vulnerability for PG that was shared with the antisocial behavior disorders, and all of the shared genetic vulnerability could be explained by the genetic risk for conduct disorder. Further analyses suggested that risk factors common to the antisocial behavior disorders and alcohol dependence accounted for 28% of the genetic variation and 8% of the individualspecific variation in PG risk; thus, most of the genetic and environmental variation in PG risk is left unexplained after accounting for the most likely sources of shared vulnerability. However, these results from the Vietnam Era Twin Study suggest that the comorbidity between PG and alcohol dependence and the antisocial behavior disorders is mainly due to genetic factors (Slutske et al., 2000, 2001).
Etiological Models
To date, a number of variables and processes have been proposed as etiological factors in PG, and several of these are described later. Because the diagnosis of PG involves a high diagnostic threshold, by the time someone’s behavior warrants the diagnosis, the individual has typically suffered considerable psychological, economic, interpersonal, and social harm. Consequently, potentially mutable variables associated with the diagnosis of PG (e.g., personality traits, affective state, biological markers) might not characterize prepathological gamblers. Because there is a dearth of detailed prospective data, we are not yet in a position to make strong claims about those variables that predispose someone to gamble problematically or pathologically.
Positive Affect Regulation (hypoarousal)
Surveys of gamblers indicate that the most commonly endorsed reason for gambling is “because it’s fun” (e.g., Wallisch, 1996). It has been suggested that individuals with PG experience and become dependent upon achieving an aroused, euphoric state similar to a drug-induced high (Griffiths, 1995; Leary & Dickerson, 1985; Lesieur & Blume, 1993; Sharpe, Tarrier, Schotte, & Spence, 1995). Experiences of wins or near-wins are hypothesized to be the stimuli that initially elicit this state of subjective and physiological arousal (Griffiths, 1991). Using the allostatic model of Koob and Le Moal (2001) described earlier, one could predict opponent processes to develop into gambling-related reinforcements that set up tolerance of gambling and, ultimately, into an allostatic process in which gambling is needed to achieve homeostatic levels of arousal.
From this general perspective, individual differences in baseline levels of arousal would be expected to be a vulnerability factor. However, individual differences in gambling behavior are not consistently related to sensation seeking, a trait that would be expected to predict reward-seeking behavior. In particular, pathological gamblers in treatment and following treatment tend to be average or even low in sensation seeking (Zuckerman, 1999). However, in active gamblers, there is a positive relation between sensation seeking and the number of gambling activities a gambler engages in, bet size, the tendency to chase losses, and loss of control (Coventry & Brown, 1993).
Zuckerman (1999) notes that measures of impulsivity tend to fare better than measures of sensation seeking in distinguishing pathological gamblers from controls. This suggests that it is not simply reward seeking but perhaps reward seeking in the context of punishment that represents a critical vulnerability to PG. For example, Newman and colleagues (e.g., Newman, Patterson, & Kosson, 1987) found that individuals with psychopathology did particularly poorly on a card-playing task when payouts are initially likely but then are manipulated to become unlikely; in such a situation, the subjects tend to play more cards and lose more money than controls because they fail to extinguish their reward-seeking behavior when the contingencies change. Using a similar task, Breen and Zuckerman (1999) found that a paper-andpencil measure of impulsivity but not sensation seeking was related to poorer task performance (i.e., losing more money).
Negative Affect Regulation
The negative-affect-regulation model of PG is embodied in the DSM-IV PG criterion “gambles as a way of escaping from problems or relieving a dysphoric mood (e.g., feelings of helplessness, guilt, anxiety, depression)” (APA, 1994, p. 618). Individuals with PG have higher rates of anxiety disorders and depression than individuals without PG, and tend to score higher on questionnaire measures of negative affectivity. In addition, depressed mood at the start of a session of gambling predicts persistence in that activity (Dickerson, Cunningham, England, & Hinchy, 1991).
There are several explanations for why gambling may help some people cope with negative emotions. Many individuals with PG describe experiencing altered states of consciousness during gambling, such as being in a trance state or feeling removed from reality (Bergh & Kuehlhorn, 1994; Bradford et al., 1996). Alternatively, gambling may help alleviate stress in some individuals by giving an illusion of control (Friedland, Keinan, & Reger, 1992). For those who are experiencing distress because of financial difficulties, gambling can serve as an active (but maladaptive) coping device that provides short-term hope for resolving these problems (Walker, 1992), and this might be particularly true of pathological gamblers with low socioeconomic status.
Deviance Proneness
The deviance proneness model emphasizes the roles of parents and peers in the development of PG. Parents are assumed to exert their influence by not providing an adequate rearing environment or by serving as gambling role models. For example, in the DSM-III (APA, 1980), the predisposing factors described for PG disorder are “loss of a parent by death, separation, divorce, or desertion before the child is 15 years of age, inappropriate parental discipline (absence, inconsistency, harshness), exposure to gambling activities as an adolescent . . . lack of family emphasis on saving, planning, and budgeting” (p. 292). Pathological gambling may be part of a constellation of associated behaviors characterized by deviance proneness or behavioral undercontrol (Stinchfield & Winters, 1998) similar to Jessor and colleagues’syndrome of problem behavior discussed earlier. For example, studies (as reviewed in Slutske et al., 2001) have shown that problem-gambling adolescents and young adults, compared to non-problem-gambling adolescents and young adults, are more likely to skip school (Wallisch, 1996), drop out of high school (Wallisch), use alcohol and other drugs (Lesieur et al., 1991; Proimos, DuRant, Pierce, & Goodman, 1998; Stinchfield, Cassuto, Winters, & Latimer, 1997; Vitaro et al., 1996; Wallisch; Winters, Stinchfield, & Fulkerson, et al., 1993), be sexually active (Proimos et al.), engage in physical fights (Proimos et al.; Vitaro et al.), have committed an illegal act or been arrested (Lesieur et al.; Stinchfield et al.; Vitaro et al.; Wallisch; West & Farrington, 1970; Winters et al.), and have friends who carry weapons or belong to gangs (Wallisch).
Cognitive Vulnerability
One set of models specific to PG, as opposed to substance use disorders, concerns specific cognitive biases that are thought to predispose an individual to gambling. Much of the research on gambling cognitions has used been based on naturalistic observations of the verbalizations of gamblers (Walker, 1992) and studies in which gamblers are asked to think out loud while they are gambling (e.g., Ladouceur & Gaboury, 1988). Based on the results of this research, several typologies of gambling-related cognitive biases have been developed (Rogers, 1998; Toneatto, 1999; Walker, 1992).
Perhaps the most familiar cognitive bias is the gambler’s fallacy or law of averages. This is the belief that the outcome of a particular bet is not independent, but rather is dependent on the outcome of previous bets. Thus, gamblers might believe that a win is more likely after a series of losses. This belief may be one mechanism that leads to chasing losses. Other biases of gamblers include a magnification of gambling skill; superstitious beliefs about how certain objects, rituals, or thoughts can increase one’s chances of winning; and more generally, the belief that the random and uncontrollable is lawful and predictable. The common theme underlying the cognitive biases engaged in by gamblers is that they help gamblers maintain optimism about the outcome of future gambling even in the face of substantial losses.
Concluding Comments
Disorders of impulse control are prevalent in our society and place high costs on the affected individuals, their friends and families, the larger community, and the criminal justice and health care systems. Because they often co-occur with each other as well as with other psychological disorders, it is important to consider them through an understanding of psychopathology in general.
These disorders often manifest themselves in youth and show developmental continuities with childhood psychopathology, and are probably related to basic temperamental proclivities. Perhaps more than other psychological disorders, their manifestation requires availability of certain types of stimuli (e.g., psychoactive substances, gambling activities), and it is thus understandable that attempts at control of these problems have often led to attempts at social control via policies that seek to restrict access to the stimulus and to impose legal sanctions on those who engage in the behavior. Although clearly certain types of environments are necessary for the development of the disorder (e.g., one can not be alcohol dependent in a culture that has effectively eliminated the making and sale of alcoholic beverages), these disorders appear to have strong genetic determinants that are likely manifested in temperamental traits such as reward seeking and self-control. The exact nature of constitutional vulnerability will probably continue to be refined in the near future.
For each of the disorders considered, there appear to be multiple etiological mechanisms that convey risk for the development of disorder. We have termed these mechanisms positive affect regulation, negative affect regulation, pharmacological vulnerability (in the case of substance use disorders), and deviance proneness. These risk mechanisms can be viewed as a starting point for developing new and refining existing approaches to prevention and treatment. Although we have emphasized similarities in the etiology and clinical manifestations of these distinct disorders, it also appears that each disorder has unique characteristics. Indeed, as implied by the multiple etiological mechanisms just mentioned, there is considerable heterogeneity within each disorder category. It seems likely that attention to underlying mechanisms will permit us to refine our diagnostic notions and derive more clearly resolved sets of diagnostic criteria.
Bibliography:
- Achenbach, T. M. (1995). Developmental issues in assessment, taxonomy, and diagnosis of child and adolescent psychopathology. In D. Cicchetti, Dante, & D. J. Cohen (Eds.), Developmental psychopathology: Vol. 1. Theory and methods (pp. 57–80). New York: Wiley.
- Achenbach, T. M., & Edelbrock, C. S. (1978). The classification of child psychopathology: A review and analysis of empirical efforts. Psychological Bulletin, 85, 1275–1301.
- Allen, J. P., Fertig, J. B., Towle, L. H., & Altshuler, V. B. (1994). Psychometric analyses of the Alcohol Dependence Scale among United States and Russian clinical samples. International Journal of the Addictions, 29, 71–87.
- Alterman,A. I., Bedrick, J., Cacciola, J. S., Rutherford, M. J., Searles, J. S., McKay, J. R., & Cook, T. G. (1998). Personality pathology and drinking in young men at high and low familial risk for alcoholism. Journal of Studies on Alcohol, 59, 495–502.
- American Psychiatric Association. (1952). Diagnostic and statistical manual of mental disorders (1st ed.). Washington, DC: Author.
- American Psychiatric Association. (1980). Diagnostic and statistical manual of mental disorders (3rd ed.). Washington, DC: Author.
- American Psychiatric Association. (1987). Diagnostic and statistical manual of mental disorders (3rd ed., rev.). Washington, DC: Author.
- American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: Author.
- American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed., Text Revision). Washington, DC: Author.
- Anthenelli, R. M., Tipp, J., Li, T. K., Magnes, L., Schuckit, M. A., Rice, J., Daw, W., & Nurnberger, J. I., Jr. (1998). Platelet monoamine oxidase activity in subgroups of alcoholics and controls: Results from the Collaborative Study on the Genetics of Alcoholism. Alcoholism: Clinical & Experimental Research, 22, 598–604.
- Anthony, J. C., & Helzer, J. (1991). Syndromes of drug abuse and dependence. In L. N. Robins & D. A. Regier (Eds.), Psychiatric disorders in America: The Epidemiologic Catchment Area Study. New York: Macmillan.
- Anthony, J. C., Warner, L. A., & Kessler, R. C. (1994). Comparative epidemiology of dependence on tobacco, alcohol, controlled substances, and inhalants: Basic findings from the National Comorbidity Survey. Experimental & Clinical Psychopharmacology, 2, 244–268.
- Babor, T. F. (1996). The classification of alcoholics: Typology theories from the nineteenth century to the present. Alcohol Health and Research World, 20(1), 6–14.
- Babor, T. F., Hofmann, M., DelBoca, F. K., Hesselbrock, V., Meyer, R. E., Dolinsky, Z. S., & Rounsaville, B. (1992). Types of alcoholics: I. Evidence for an empirically derived typology based on indicators of vulnerability and severity. Archives of General Psychiatry, 49, 599–608.
- Barnes, G. E. (1983). Clinical and prealcoholic personality characteristics. In B. Kissin & H. Begleiter (Eds.), The pathogenesis of alcoholism: Psychosocial factors (pp. 113–195). New York: Plenum Press.
- Bates, M. E., & Labouvie, E. W. (1995). Personality environment constellations and alcohol use: A process-oriented study of intraindividual change during adolescence. Psychology of Addictive Behaviors, 9, 23–35.
- Bergh, C., & Kuehlhorn, E. (1994). The development of pathological gambling in Sweden. Journal of Gambling Studies, 10, 261–274.
- Bergler, E. (1936). Psychology of the gambler. Imago (Leipzig), 22, 409–441.
- Bergler, E. (1943). The gambler: Amisunderstood neurotic. Journal of Criminal Psychopathology, 4, 379–393.
- Bergler, E. (1957). The psychology of gambling. Madison, CT: International Universities Press.
- Bergman, B., & Brismar, B. (1994). Hormone levels and personality traits in abusive and suicidal male alcoholics. Alcoholism: Clinical and Experimental Research, 18, 311–316.
- Black, D. W., & Moyer, T. (1998). Clinical features and psychiatric comorbidity of subjects with pathological gambling behavior. Psychiatric Services, 49, 1434–1439.
- Blanco, C., Orensanz-Munoz, L., Blanco-Jerez, C., & Saiz-Ruiz, J. (1996). Pathological gambling and platelet MAO activity: A psychobiological study. American Journal of Psychiatry, 153, 119–121.
- Bland, R. C., Newman, S. C., Orn, H., & Stebelsky, G. (1993). Epidemiology of pathological gambling in Edmonton. Canadian Journal of Psychiatry, 38, 108–112.
- Blaszczynski,A.P.,Buhrish,N.,&McConaghy,N.(1985).Pathologicalgamblers,heroinaddicts,andcontrolscomparedontheE.P.Q. “Addiction Scale.” British Journal of Addiction, 80, 315–319.
- Blaszczynski, A., & Farrell, E. (1998). Acase series of 44 completed gambling-related suicides. Journal of Gambling Studies, 14, 93–109.
- Blaszczynski, A., Hyde, J., & Sandanam, J. (1991). Pathological gambling secondary to brain trauma: A case study. Journal of Gambling Studies, 7, 65–71.
- Blaszczynski, A., & Silove, D. (1996). Pathological gambling: Forensic issues. Australian and New Zealand Journal of Psychiatry, 30, 358–369.
- Blaszczynski, A., & Steel, Z. (1998). Personality disorders among pathological gamblers. Journal of Gambling Studies, 14, 51–71.
- Blaszczynski, A., Steel, Z., & McConaghy, N. (1997). Impulsivity in pathological gambling: The antisocial impulsivist. Addiction, 92, 75–87.
- Blaszczysnski, A. P., Wilson, A. C., & McConaghy, N. (1986). Sensation seeking and pathological gambling. British Journal of Addiction, 81, 113–117.
- Bonnie, R., & Whitebread, C. (1974). The marijuana conviction: A history of marijuana prohibition in the United States. New York: Lindesmith Center.
- Bowman, K. M., & Jellinek, E. M. (1941). Alcoholic mental disorders. Quarterly Journal of Studies on Alcohol, 2, 312–390.
- Bradford, J., Geller, J., Lesieur, H. R., Rosenthal, R., & Wise, M. (1996). Impulse control disorders. In T. A. Widiger, A. J. Frances, H. A. Pincus, R. Ross, M. B. First, & D. W. Wakefield (Eds.), DSM-IV sourcebook: Vol. 2. Washington, DC: American Psychiatric Association.
- Breen, R. B., & Zuckerman, M. (1999). “Chasing” in gambling behavior: Personality and cognitive determinants. Personality & Individual Differences, 27, 1097–1111.
- Breslin, F. C., Sobell, M. B., Cappell, H., Vakili, S., & Poulos, C. X. (1999). The effects of alcohol, gender, and sensation seeking on the gambling choices of social drinkers. Psychology of Addictive Behaviors, 13, 243–252.
- Bucholz,K.K.,Heath,A.C.,Reich,T.,&Hesselbrock,V.M.(1996). Can we subtype alcoholism? A latent class analysis of data from relativesofalcoholicsinamulticenterfamilystudyofalcoholism. Alcoholism: Clinical & Experimental Research, 20, 1462–1471.
- Cappell, H., & Herman, C. P. (1972). Alcohol and tension reduction. Areview. Quarterly Journal of Studies on Alcohol, 33, 33–64.
- Carrasco, J. L., Saiz-Ruiz, J., Hollander, E., Cesar, J., & Lopez-Ibor, J. J., Jr. (1994). Low platelet monoamine oxidase activity in pathological gambling. Acta Psychiatrica Scandinavica, 90, 427–431.
- Caspi,A.,Begg,D.,Dickson,N.,Harrington,H.,Langley,J.,Moffitt, T.E.,&Silva,P.A.(1997).Personalitydifferencespredicthealthrisk behaviors in young adulthood: Evidence from a longitudinal study. Journal of Personality & Social Psychology, 73, 1052– 1063.
- Caspi, A., & Moffitt, T. E. (1995). The continuity of maladaptive behavior: From description to understanding in the study of antisocial behavior. In D. Cicchetti & D. J. Cohen (Eds.), Developmental psychopathology: Vol. 2. Risk, disorder, and adaptation (pp. 472–511). New York: Wiley. de Castro, I. P., Ibanez, A., Saiz-Ruiz, J., & Fernandez, P. J. (1999). Genetic contribution to pathological gambling: Possible association between a functional DNA polymorphism at the serotonin transporter gene (5-HTT) and affected men. Pharmacogenetics, 9, 397–400.
- Chassin, L., Curran, P. J., Hussong, A. M., & Colder, C. R. (1996). The relation of parent alcoholism to adolescent substance use: A longitudinal follow-up study. Journal of Abnormal Psychology, 105, 70–80.
- Chen, K., & Kandel, D. B. (1995). The natural history of drug use from adolescence to the mid-thirties in a general population sample. American Journal of Public Health, 85, 41–47.
- Ciarrocchi, J. W., Kirschner, N. M., & Fallik, F. (1991). Personality dimensions of male pathological gamblers, alcoholics, and dually addicted gamblers. Journal of Gambling Studies, 7, 133– 141.
- Cloninger, C. R. (1987a). Neurogenetic adapative mechanisms in alcoholism. Science, 236, 410–416.
- Cloninger, C. R. (1987b). A systematic method for clinical description and classification of personality variants. Archives of General Psychiatry, 44, 573–588.
- Cloninger, C. R. (1987c). Tridimensional Personality Questionnaire, version 4. Unpublished manuscript.
- Cloninger, C. R., Sigvardsson, S., Reich, T., & Bohman, M. (1988). Childhood personality predicts alcohol abuse in young adults. Alcoholism: Clinical and Experimental Research, 12, 494–505.
- Comings, D. E., Gonzalez, N., Wu, S., Gade, R., Muhleman, D., Saucier,G.,Johnson,P.,Verde,R.,Rosenthal,R.J.,Lesieur,H. R., Rugle, L. J., Miller, W. B., & MacMurray, J. P. (1999). Studies of the 48 bp repeat polymorphism of the DRD4 gene in impulsive, compulsive, addictive behaviors: Tourette Syndrome, ADHD, pathological gambling, and substance abuse. American Journal of Medical Genetics (Neuropsychiatric Genetics), 88, 358–368.
- Comings, D. E., Rosenthal, R. J., Lesieur, H. R., Rugle, L. J., Muhleman, D., Chiu, C., Dietz, G., & Gade, R. (1996). A study of the dopamine D2 receptor gene in pathological gambling. Pharmacogenetics, 6, 223–234.
- Cooper, M. L., Frone, M. R., Russell, M., & Mudar, P. (1995). Drinking to regulate positive and negative emotions: A motivational model of alcohol use. Journal of Personality & Social Psychology, 69, 990–1005.
- Cooper, M. L., Russell, M., Skinner, J. B., & Windle, M. (1992). Development and validation of a three-dimensional measure of drinking motives. Psychological Assessment, 4, 123–132.
- Costello, E. J., Erkanli, A., Federman, E., & Angold, A. (1999). Development of psychiatric comorbidity with substance abuse in adolescents: Effects of timing and sex. Journal of Clinical Child Psychology, 28, 298–311.
- Cotton, N. (1979). The familial incidence of alcoholism: A review. Journal of Studies on Alcohol, 40, 89–116.
- Coventry, K. R., & Brown, R. I. (1993). Sensation seeking, gambling and gambling addictions. Addiction, 88, 541–554.
- Cox, W. M. (1987). Personality theory and research. In H. T. Blane & K. E. Leonard (Eds.), Psychological theories of drinking and alcoholism (pp. 55–84). New York: Guilford Press.
- Crockford, D. N., & el-Guebaly, N. (1998). Psychiatric comorbidity in pathological gambling: Acritical review. Canadian Journal of Psychiatry, 43, 43–50.
- Cunningham-Williams, R. M., Cottler, L. B., Compton, W. M., III, & Spitznagel, E. L. (1998). Taking chances: Problem gamblers and mental health disorders: Results from the St. Louis Epidemiologic Catchment Area study. American Journal of Public Health, 88, 1093–1096.
- Cunningham-Williams, R. M., Cottler, L. B., Compton, W. M., Spitznagel, E. L., & Ben-Abdallah, A. (2000). Problem gambling and comorbid psychiatric and substance use disorders among drug users recruited from drug treatment and community settings. Journal of Gambling Studies, 16, 347–376.
- Dell, L., Ruzicka, M., & Palisi, A. (1981). Personality and other factors associated with the gambling addiction. International Journal of the Addictions, 16, 149–156.
- Diamond, I., & Gordon, A. (1995). Biochemical phenotypic markers in genetic alcoholism. In H. Begleiter & B. Kissin (Eds.), Alcohol and alcoholism: Vol. 1. The genetics of alcoholism (pp. 259–268). New York: Oxford University Press.
- Dickerson, M., & Baron, E. (2000). Contemporary issues and future directions for research into pathological gambling. Addiction, 95, 1145–1159.
- Dickerson, M., Cunningham, R., England, S. L., & Hinchy, J. (1991). On the determinants of persistent gambling: III. Personality, prior mood, and poker machine play. International Journal of the Addictions, 26, 531–548.
- Dishion, T. J., French, D. C., & Patterson, G. R. (1995). The development and ecology of antisocial behavior. In D. Cicchetti & D. J. Cohen (Eds.), Developmental psychopathology: Vol. 2. Risk, disorder, and adaptation (pp. 421–471). New York: Wiley.
- Donovan, J. E., & Jessor, R. (1985). Structure of problem behavior in adolescence and young adulthood. Journal of Consulting and Clinical Psychology, 53, 890–904.
- Donovan, J. E., Jessor, R., & Costa, F. M. (1988). Syndrome of problem behavior in adolescence: A replication. Journal of Consulting and Clinical Psychology, 56, 762–765.
- Earleywine, M., & Finn, P. R. (1991). Sensation seeking explains the relation between behavioral disinhibition and alcohol consumption. Addictive Behaviors, 16, 123–128.
- Edwards, G. (1982). The treatment of drinking problems: A guide for the helping professions. New York: McGraw-Hill.
- Edwards, G. (1986). The alcohol dependence syndrome: A concept as stimulus to enquiry. British Journal of Addiction, 81, 171–183.
- Edwards, G., & Gross, M. (1976). Alcohol dependence: Provisional decription of a clinical syndrome. British Medical Journal, 1, 1058–1061.
- Eisen, S. A., Lin, N., Lyons, M. J., Scherrer, J. F., Griffith, K., True, W. R., Goldberg, J., & Tsuang, M. T. (1998). Familial influences on gambling behavior: An analysis of 3359 twin pairs. Addiction, 93, 1375–1384.
- Feighner, J. P., Robins, E., Guze, S. B., Woodruff, R. A., Winokur, G., & Munoz, R. (1972). Diagnostic criteria for use in psychiatric research. Archives of General Psychiatry, 26, 57–63.
- Fere,C.(1899).Thepathologyofemotions(R.Park,Trans.).London: University Press.
- Freud, S. (1961). Dostoevsky and parricide. In J. Strachey (Ed. & Trans.), Standard edition of the complete psychological works of Sigmund Freud (Vol. 21, pp. 175–196). London: Hogarth. (Original work published 1928)
- Friedland, N., Keinan, G., & Regev, Y. (1992). Controlling the uncontrollable: Effects of stress on illusory perceptions of controllability. Journal of Personality and Social Psychology, 63, 923–931.
- Fromme, K., Katz, E., & D’Amico, E. (1997). Effects of alcohol intoxication on the perceived consequences of risk taking. Experimental and Clinical Psychopharmacology, 5, 14–23.
- Fromme, K., Stroot, E. A., & Kaplan, D. (1993). Comprehensive effects of alcohol: Development and psychometric assessment of a new expectancy questionnaire. Psychological Assessment, 5, 19–26.
- Gambino, B., Fitzgerald, R., Shaffer, H. J., & Renner, J. (1993). Perceived family history of problem gambling and scores on SOGS. Journal of Gambling Studies, 9, 169–184.
- Gerstein, D., Volberg, R., Hoffmann, J., Larison, C., Engelman, L., Murphy, S., Palmer, A., Chuchro, L., Toce, M., Johnson, R., Buie, T., & Hill, M. A. (1999). Gambling impact and behavior study. New York: Christiansen/Cummings Associates.
- Giacopassi, D., Stitt, B. G., & Vandiver, M. (1998). An analysis of the relationship of alcohol to casino gambling among college students. Journal of Gambling Studies, 14, 135–149.
- Gianoulakis, C. (1996). Implications of endogenous opioids and dopamine in alcoholism: Human and basic science studies. Alcohol & Alcoholism, 31, 33–42.
- Goldman, M. S., Del Boca, F. K., & Darkes, J. (1999). Alcohol expectancy theory: The application of cognitive neuroscience. In K. E. Leonard & H. T. Blane (Eds.), Psychological theories of drinking and alcoholism (2nd ed., pp. 203–246). New York: Guilford Press.
- Goode, E. (1999). Drugs in American society (5th ed.). New York: McGraw-Hill.
- Gorenstein, E. E. (1987). Cognitive-perceptual deficit in an alcoholism spectrum disorder. Journal of Studies on Alcohol, 48, 310–318.
- Gorenstein, E. E., & Newman, J. P. (1980). Disinhibitory psychopathology: A new perspective and a model for research. Psychological Review, 87, 301–315.
- Graham, J. R., & Lowenfeld, B. H. (1986). Personality dimensions of the pathological gambler. Journal of Gambling Behavior, 2, 58–66.
- Grant, B. F. (1997). Prevalence and correlates of alcohol use and DSM-IV alcohol dependence in the United States: Results of the National Longitudinal Alcohol Epidemiologic Survey. Journal of Studies on Alcohol, 58, 464–473.
- Grant, B. F., Harford, T., Dawson, D., Chou, P., Dufour, M., & Pickering, R. (1994). Prevalence of DSM-IV alcohol abuse and dependence. Alcohol Health and Research World, 18, 243–248.
- Grant, B. F., & Pickering, R. P. (1996). Comorbidity between DSM-IV alcohol and drug use disorders: Results from the National Longitudinal Alcohol Epidemiologic Survey. Alcohol Health & Research World, 20(1), 67–72.
- Greeley, J., & Oei, T. (1999). Alcohol and tension reduction. In K. Leonard & H. T. Blane (Eds.), Psychological theories of drinking and alcoholism (2nd ed., pp. 14–53). New York: Guilford Press.
- Griffiths, M. D. (1991). Psychobiology of the near-miss in fruit machine gambling. Journal of Psychology, 125, 347–357.
- Griffiths, M. D. (1995). The role of subjective mood states in the maintenance of fruit machine gambling behaviour. Journal of Gambling Studies, 11, 123–135.
- Gupta, R., & Derevensky, J. (1997). Familial and social influences on juvenile gambling behavior. Journal of Gambling Studies, 13, 179–192.
- Hand, I. (1998). Pathological gambling: A negative state model and its implications for behavioral treatments. CNS Spectrums, 3, 58–71.
- Harada, S., Agarwal, D. P., Goedde, H. W., Tagaki, S., & Ishikawa, B. (1982). Possible protective role against alcoholism for aldehyde dehydrogenase isozyme deficiency in Japan. Lancet, 2(8302), 827.
- Hare, R. D. (1984). Performance of psychopaths on cognitive tasks related to frontal lobe function. Journal of Abnormal Psychology, 93, 133–140.
- Hasin, D. S., Muthen, B., Wisnicki, K. S., & Grant, B. (1994). Validity of the bi-axial dependence concept: A test in the U.S. general population. Addiction, 89, 573–579.
- Hawkins, J. D., Catalano, R. F., & Miller, J. Y. (1992). Risk and protective factors for alcohol and other drug problems in adolescence and early adulthood: Implications for substance abuse prevention. Psychological Bulletin, 112, 64–105.
- Heath, A. C. (1995a). Genetic influences on alcoholism risk: A review of adoption and twin studies. Alcohol Health and Research World, 19(3), 166–171.
- Heath, A. C. (1995b). Genetic influences on drinking behavior in humans. In H. Begleiter & B. Kissin (Eds.), Alcohol and alcoholism: Vol. 1. The genetics of alcoholism (pp. 82–121). New York: Oxford University Press, Inc.
- Heath, A. C., Bucholz, K. K., Madden, P. A. F., Dinwiddie, S. H., Slutske, W. S., Bierut, L. J., Statham, D. J., Dunne, M. P., Whitfield, J., & Martin, N. G. (1997). Genetic and environmental contributions to alcohol dependence risk in a national twin sample: Consistency of findings in women and men. Psychological Medicine, 27, 1381–1396.
- Heath, A. C., Bucholz, K. K., Slutske, W. S., & Madden, P. A. F. (1994). The assessment of alcoholism in surveys of the general community: What are we measuring? Some insights from the Australian twin panel interview survey. International Review of Psychiatry, 6, 295–307.
- Helzer, J. E., Burnam, A., & McEvoy, L. T. (1991). Alcohol abuse and dependence. In L. N. Robins & D. A. Regier (Eds.), Psychiatric disorders in America: The Epidemiologic Catchment Area Study (pp. 81–115). New York: Macmillan.
- Helzer, J. E., & Canino, G. J. (Eds.). (1992). Alcoholism in North America, Europe, and Asia. New York: Oxford University Press.
- Helzer, J. E., & Pryzbeck, T. R. (1988). The co-occurrence of alcoholism with other psychiatric disorders in the general population and its impact on treatment. Journal of Studies on Alcohol, 49, 219–224.
- Hesselbrock, V. M. (1995). The genetic epidemiology of alcoholism. In H. Begleiter & B. Kissin (Eds.), Alcohol and alcoholism: Vol. 1. The genetics of alcoholism (pp. 17–39). New York: Oxford University Press.
- Holdcraft, L. C., Iacono, W. G., & McGue, M. K. (1998). Antisocial Personality Disorder and depression in relation to alcoholism: A community-based sample. Journal of Studies on Alcohol, 59, 222–226.
- Horgan,C.,Skwara,K.,&Strickler,G.(2001).Substanceabuse:The nation’s number one health problem. Princeton, NJ: Schneider Institute for Health Policy, Brandeis University.
- Institute of Medicine. (1990). Broadening the base of treatment for alcohol problems. Washington, DC: NationalAcademy Press.
- Jackson, K. M., Sher, K. J., & Wood, P. K. (2000). Prospective analysis of comorbidity: Tobacco and alcohol use disorders. Journal of Abnormal Psychology, 109, 679–694.
- Jang, K. L., Vernon, P. A., & Livesley, W. J. (2000). Personality disorder traits, family environment, and alcohol misuse: A multivariate behavioural genetic analysis. Addiction, 95, 873–888.
- Jellinek, E. M. (1960). The disease concept of alcoholism. New Haven, CT: Hillhouse.
- Jessor, R., Donovan, J. E., & Costa, F. M. (1991). Beyond adolescence: Problem behavior and young adult development. New York: Cambridge University Press.
- Jessor, R., & Jessor, S. (1977). Problem behavior and psychosocial development: A longitudinal study of youth. New York: Academic Press.
- Jones, M. C. (1968). Personality correlates and antecedents of drinking patterns in adult males. Journal of Consulting & Clinical Psychology, 32, 2–12.
- Kadden, R. M., Kranzler, H. R., & Rounsaville, B. J. (1995). Validity of the distinction between “substance-induced” and “independent” depression and anxiety disorders. American Journal on Addictions, 4, 107–117.
- Kaplan, H. B. (1975). Increase in self-rejection as an antecedent of deviant responses. Journal of Youth and Adolescence, 4, 281– 292.
- Keller, M., & Doria, J. (1991). On defining alcoholism. Alcohol Health & Research World, 15, 253–259.
- Kendler, K., Karkowski, L., Corey, L., Prescott, C., & Neale, M. (1999). Genetic and environmental risk factors in the atiology of illicit drug initiation and subsequent misuse in women. The British Journal of Psychiatry, 175, 351–356.
- Kendler, K. S., Karkowski, L., Neale, M., & Prescott, C. (2000). Illicit psychoative substance use, heavy use, abuse, and dependence in a US population-based sample of male twins. Archives of General Psychiatry, 57, 261–269.
- Kendler,K.S.,Karkowski,L.,&Prescott,C.A.(1999).Hallucinogen, opiate, sedative and stimulant use and abuse in a population-based sample of female twins. Acta Psychiatrica Scandinavica, 99, 368–376.
- Kendler, K. S., & Prescott, C. A. (1998a). Cannabis use, abuse, and dependence in a population-based sample of female twins. American Journal of Psychiatry, 155, 1016–1022.
- Kendler, K. S., & Prescott, C. A. (1998b). Cocaine use, abuse and dependence in a population-based sample of female twins. British Journal of Psychiatry, 173, 345–350.
- Kendler, K. S., Walters, E. E., Neale, M. C., Kessler, R. C., Heath, A. C., & Eaves, L. J. (1995). The structure of the genetic and environmental risk factors for six major psychiatric disorders in women: Phobia, generalized anxiety disorder, panic disorder, bulimia, major depression and alcoholism. Archives of General Psychiatry, 52, 374–383.
- Kessler, R. C., Crum, R. M., Warner, L. A., & Nelson, C. B. (1997). Lifetime co-occurrence of DSM-III-R alcohol abuse and dependence with other psychiatric disorders in the National Comorbidity Survey. Archives of General Psychiatry, 54, 313–321.
- Kessler, K., McGonagle, K., Zhao, S., Nelson, C., Hughes, M., Eshleman, S., Wittchen, H., & Kendler, K. (1994). Lifetime and 12 month prevalence of DSM-III-R psychiatric disorders in the United States. Archives of General Psychiatry, 51, 8–19.
- Kilbey, M. M., Downey, K., & Breslau, N. (1998). Predicting the emergence and persistence of alcohol dependence in young adults: The role of expectancy and other risk factors. Experimental & Clinical Psychopharmacology, 6, 149–156.
- King, R. (1972). The drug hang-up: America’s fifty year folly. New York: W. W. Norton.
- Klein, D. N., & Riso, L. P. (1993). Psychiatric disorders: Problems of boundaries and comorbidity. In C. G. Costello (Ed.), Basic issues in psychopathology (pp. 19–66). New York: Guilford Press.
- Knight, R. P. (1938). The psychoanalytic treatment in a sanatorium of chronic addiction to alcohol. Journal of the American Medical Association, 111, 1443–1448.
- Koob, G. (2000). Drug addiction. Neurobiology of Disease, 7, 543–545.
- Koob, G. F., & Le Moal, M. (2001). Drug addiction, dysregulation of reward, and allostasis. Neuropsychopharmacology, 24, 97–129.
- Kreitman, N. (1986). Alcohol consumption and the preventive paradox. British Journal of Addiction, 81, 353–363.
- Krueger, R. F. (1999). The structure of common mental disorders. Archives of General Psychiatry, 56, 921–926.
- Krueger, R. F., Caspi, A., Moffitt, T. E., & Silva, P. A. (1998). The structure and stability of common mental disorders (DSM-III-R): A longitudinal-epidemiological study. Journal of Abnormal Psychology, 107, 216–227.
- Kuhn, C., Swartzwalder, S., & Wilson, W. (1998). Buzzed: The straight facts about the most used and abused drugs from alcohol to ecstasy. New York: W. W. Norton.
- Kushner, M. G., Sher, K. J., & Erickson, D. J. (1999). Prospective analysis of the relation between DSM-III anxiety disorders and alcohol use disorders. American Journal of Psychiatry, 156, 723–732.
- Kyngdon, A., & Dickerson, M. (1999). An experimental study of the effect of prior alcohol consumption on a simulated gambling activity. Addiction, 94, 697–707.
- Labouvie, E. W., Pandina, R. J., White, H. R., & Johnson, V. (1990). Risk factors of adolescent drug use: An affect-based interpretation. Journal of Substance Abuse, 2, 265–285.
- Ladouceur, R., & Gaboury, A. (1988). Effects of limited and unlimited stakes on gambling behavior. Journal of Gambling Behavior, 4,
- Langenbucher, J., Martin, C. S., Labouvie, E., Sanjuan, P. M., Bavly, L., & Pollock, N. K. (2000). Toward the DSM-V: The withdrawal-gate model versus the DSM-IV in the diagnosis of alcohol abuse and dependence. Journal of Consulting & Clinical Psychology, 68, 799–809.
- Leary, K., & Dickerson, M. G. (1985). Levels of arousal in high and low frequency gamblers. Behavior Research and Therapy, 23, 635–640.
- LeMarquand, D. G., Benkelfat, C., Pihl, R. O., Palmour, R. M., & Young, S. N. (1999). Behavioral disinhibition induced by tryptophan depletion in nonalcoholic young men with multigenerational family histories of paternal alcoholism. American Journal of Psychiatry, 156, 1771–1779.
- Lesieur, H. R. (1984). The chase: Career of the compulsive gambler. Rochester, VT: Schenkman Books.
- Lesieur, H. R., & Blume, S. B. (1993). Pathological gambling, eating disorders, and the psychoactive substance use disorders. Journal of Addictive Diseases, 12, 89–102.
- Lesieur, H. R., Blume, S. B., & Zoppa, R. M. (1986). Alcoholism, drug abuse, and gambling. Alcoholism: Clinical & Experimental Research, 10, 33–38.
- Lesieur, H. R., Cross, J., Frank, M., Welch, M., White, C. M., Rubenstein, G., Moseley, K., & Mark, M. (1991). Gambling and pathological gambling among university students. Addictive Behaviors, 16, 517–527.
- Lichtermann, D., Hranilovic, D., Trixler, M., Franke, P., Jernej, B., Delmo, C. D., Knapp, M., Schwab, S. G., Maier, W., & Wildenauer, D. B. (2000). Support for allelic association of a polymorphic site in the promoter region of the serotonin transporter gene with risk for alcohol dependence. American Journal of Psychiatry, 157, 2045–2047.
- Linden, R. D., Pope, H. G., & Jonas, J. M. (1986). Pathological gambling and major affective disorder: Preliminary findings. Journal of Clinical Psychiatry, 47, 201–203.
- Linnoila, M., Virkkunen, M., George, T., & Higley, D. (1993). Impulse control disorders. International Clinical Psychopharmacology, 8, 53–56.
- Litten, R. Z., & Allen, J. P. (1998). Advances in development of medications for alcoholism treatment. Psychopharmacologia, 139, 20–33.
- Luria, A. R. (1980). Neuropsychology in the local diagnosis of brain damage. International Journal of Clinical Neuropsychology, 2, 1–7.
- Lyons, M. J., Eisen, S. A., Goldberg, J., True, W., Lin, N., Meyer, M., Toomey, R., Faraone, S. V., Merla-Ramos, M., & Tsuang, M. T. (1998). A registry-based twin study of depression in men. Archives of General Psychiatry, 55, 468–472.
- Major, L. F., & Murphy, D. L. (1978). Platelet and plasma amine oxidase activity in alcoholic individuals. British Journal of Psychiatry, 132, 548–554.
- McCormick, R. S., Taber, J., Kruedelbach, N., & Russo, A. (1987). Personality profiles of hospitalized pathological gamblers: The California Personality Inventory. Journal of Clinical Psychology, 43, 521–572.
- McGue, M. (1999). Behavioral genetic models of alcoholism and drinking. In K. E. Leonard & H. T. Blane (Eds.), Psychological theories of drinking and alcoholism (2nd ed., pp. 372–421). New York: Guilford Press.
- Merikangas, K. R., Stevens, D. E., Fenton, B., Stolar, M., O’Malley, S., Woods, S. W., & Risch, N. (1998). Co-morbidity and familial aggregation of alcoholism and anxiety disorders. Psychological Medicine, 28, 773–788.
- Molina, B. S. G., Chassin, L., & Curran, P. J. (1994). A comparison of mechanisms underlying substance use for early adolescent children of alcoholics and controls. Journal of Studies on Alcohol, 55, 269–275.
- Morgan, A. B., & Lilienfeld, S. O. (2000). Ameta-analytic review of the relation between antisocial behavior and neuropsychological measures of executive function. Clinical Psychology Review, 20, 113–136.
- Muthen, B. O., Grant, B., & Hasin, D. (1993). The dimensionality of alcohol abuse and dependence: Factor analysis of DSM-III-R and proposed DSM-IV criteria in the 1988 National Health Interview Survey. Addiction, 88, 1079–1090.
- Nathan, P. (1988). The addictive personality is the behavior of the addict. Journal of Consulting and Clinical Psychology, 56, 183–188.
- (1972).Criteriaforthediagnosisof alcoholism. American Journal of Psychiatry, 129, 127–135.
- National Council on Alcoholism, Criteria Committee. (1972). Criteria for the diagnosis of alcoholism. Annals of Internal Medicine, 77, 249–258.
- National Institute on Alcohol Abuse and Alcoholism. (2000). 10th special report to the U.S. Congress on alcohol and health. Washington, DC: U.S. Department of Health and Human
- National Research Council. (1999). Pathological gambling: A critical review. Washington, DC: National Academy Press.
- Nelson, C. B., Heath, A. C., & Kessler, R. C. (1998). Temporal progression of alcohol dependence symptoms in the U.S. household population: Results from the National Comorbidity Survey. Journal of Consulting & Clinical Psychology, 66, 474–483.
- Newlin, D. B., & Thomson, J. B. (1990). Alcohol challenge with sons of alcoholics: A critical review and analysis. Psychological Bulletin, 108, 383–402.
- Newman, J. P., Patterson, C. M., & Kosson, D. S. (1987). Response preservation in psychopaths. Journal of Abnormal Psychology, 96, 145–148.
- Nigg, J. T. (2000). On inhibiton/disinhibition in development psychopathology: Views from cognitive and personality psychology and a working inhibition taxonomy. Psychological Bulletin, 126, 220–246.
- Noll, R. B., Zucker, R. A., & Greenberg, G. S. (1990). Identification of alcohol by smell among preschoolers: Evidence for early socialization about drugs occurring in the home. Child Development, 61, 1520–1527.
- Oetting, E. R., & Beauvais, F. (1986). Peer cluster theory: Drugs and the adolescent. Journal of Counseling & Development, 65, 17–22.
- O’Neill, S., & Sher, K. J. (2000). Physiological alcohol dependence symptoms in early adulthood: Alongitudinal perspective. Experimental and Clinical Psychopharmacology, 8, 493–508.
- Orford, J. (2001). Addiction as excessive appetite. Addiction, 96, 15–31.
- Pederson, W. (1991). Mental health, sensation seeking and drug use patterns: A longitudinal study. British Journal of Addiction, 86, 195–204.
- Petraitis, J., Flay, B. R., & Miller, T. Q. (1995). Reviewing theories of adolescent substance use: Organizing pieces in the puzzle. Psychological Bulletin, 117, 67–86.
- Petry, N. M., & Armentano, C. (1999). Prevalence, assessment, and treatment of pathological gambling: A review. Psychiatric Services, 50, 1021–1027.
- Pettinati, H. M., Volpicelli, J. R., Luck, G., Kranzler, H. R., Rukstalis, M. R., & Cnaan, A. (2001). Double-blind clinical trial of sertraline treatment for alcohol dependence. Journal of Clinical Psychopharmacology, 21, 143–153.
- Phillips, D. P., Welty, W. R., & Smith, M. M. (1997). Evaluated suicide levels associated with legalized gambling. Suicide & LifeThreatening Behavior, 27, 373–378.
- Pihl, R. O., & Bruce, K. R. (1995). Cognitive impairment in children of alcoholics. Alcohol Health and Research World, 19(2), 142–147.
- Plutchik, A., & Plutchik, R. (1988). Psychosocial correlates of alcoholism. Integrative Psychiatry, 6, 205–210.
- Polich, J., Pollock, V. E., & Bloom, F. E. (1994). Meta-analysis of P300 amplitude from males at risk for alcoholism. Psychological Bulletin, 115, 55–73.
- Pollock, V. E. (1992). Meta-analysis of subjective sensitivity to alcohol in sons of alcoholics. American Journal of Psychiatry, 149, 1534–1538.
- Poznanski, A. (1959). Our drinking heritage. In R. G. McCarthy (Ed.), Drinking and intoxication: Selected reading in social attitudes and controls (pp. 42–43). New Haven, CT: College and University Press.
- Prescott, C. A., Aggen, S. H., & Kendler, K. S. (2000). Sex-specific genetic influences on the comorbidity of alcoholism and major depression in a population-based sample of US twins. Archives of General Psychiatry, 57, 803–811.
- Prescott, C. A., Neale, M. C., Corey, L. A., & Kendler, K. S. (1997). Predictors of problem drinking and alcohol dependence in a population-based sample of female twins. Journal of Studies on Alcohol, 58, 167–181.
- Productivity Commission. (1999). Australia’s gambling industries (Inquiry Report, Vol. 1, No. 10).
- Proimos, J., DuRant, R. H., Pierce, J. D., & Goodman, E. (1998). Gambling and other risk behaviors among 8th- to 12th-grade students. Pediatrics, 102,
- Ramirez, L., McCormick, R., Russo, A., & Taber, J. (1983). Patterns of substance abuse in pathological gamblers undergoing treatment. Addictive Behaviors, 8, 425–428.
- Rankin, H., Stockwell, T., & Hodgson, R. (1982). Personality and alcohol dependence. Personality & Individual Differences, 3, 145–151.
- Reich, T., Cloninger, C. R., Van Eerdewegh, P., Rice, J. P., & Mullaney, J. (1988). Secular trends in the familial transmission of alcoholism. Alcoholism: Clinical & Experimental Research, 12, 458–464.
- Reich, T., Edenberg, H. J., Goate, A., Williams, J. T., Rice, J. P., Van Eerdewegh, P., Foroud, T., Hesselbrock, V., Schuckit, M. A., Bucholz, K. K., Porjesz, B., Li, T. K., Conneally, P. M., Nurnberger, J. I., Jr., Tischfield, J. A., Crowe, R. R., Cloninger, R., Wu, W., Shears, S., Carr, K., Crose, C., Willig, C., & Begleiter, H. (1998). Genome-wide search for genes affecting the risk for alcohol dependence. American Journal of Medical Genetics, 81, 207–215.
- Regier, D. A., Farmer, M. E., Rae, D. S., Locke, B. Z., Keith, S. J., Judd, L. L., & Goodwin, F. K. (1990). Comorbidity of mental disorders with alcohol and other drug abuse: Results from the Epidemiologic Catchment Area (ECA) Study. Journal of American Medical Association, 264, 2511–2518.
- Repo, E., Kuikka, J. T., Bergstroem, K. A., Karhu, J., Hiltunen, J., & Tiihonen, J. (1999). Dopamine transporter and D-sub-2-receptor density in late-onset alcoholism. Psychopharmacology, 147, 314–318.
- Robins, L., Bates, W., & O’Neal, P. (1962). Adult drinking patterns of former problem children. In D. Pittman & C. R. Synder (Eds.), Society, culture, and drinking patterns (pp. 395–412). New York: Wiley.
- Robins, L. N., Bates, W. M., & O’Neal, P. (1991). Adult drinking patterns of former problem children. In D. Pittman & H. R.White (Eds.), Society, culture, and drinking patterns reexamined. Alcohol, culture, and social control monograph series (pp. 460–479). Piscataway, NJ: Rutgers Center of Alcohol Studies.
- Rogers, P. (1998). The cognitive psychology of lottery gambling: A theoretical review. Journal of Gambling Studies, 14, 111–134.
- Roy, A., Adinoff, B., Roehrich, L., Lamparski, D., Custer, R., Lorenz, V., Barbaccia, M., Guidotti, A., Costa, E., & Linnoila, M. (1988). Pathological gambling. Archives of General Psychiatry, 45, 369–373.
- Sayette, M. A. (1999). Does drinking reduce stress? Alcohol Health and Research World, 23(4), 250–255.
- Schooler, C., Zahn, T. P., Murphy, D. L., & Buchsbaum, M. S. (1978). Psychological correlates of monoamie oxidase in normals. Journal of Nervous and Mental Disease, 166, 177–186.
- Schuckit, M. A. (1985). Genetics and the risk for alcoholism. Journal of the American Medical Association, 253, 2614–2617.
- Schuckit, M. A. (1994). The relationship between alcohol problems, substance abuse and psychiatric problems. In T. A. Widiger, A. J. Frances, H. A. Pincus, M. B. First, R. Ross, & W. Davis (Eds.), DSM-IV sourcebook (Vol. 1, pp. 45–66). Washington, DC: American Psychiatric Association.
- Schuckit, M. A. (1998). Biological, psychological and environmental predictors of the alcoholism risk: A longitudinal study. Journal of Studies on Alcohol, 59, 485–494.
- Schuckit, M. A., & Smith, T. L. (1996). An 8-year follow-up of 450 sons of alcoholic and control subjects. Archives of General Psychiatry, 53, 202–210.
- Schuckit, M. A., Smith, T. L., Daeppen, J. B., Eng, M., Li, T. K., Hesselbrock,V.M.,Nurnberger,J.I.,Jr.,&Bucholz,K.K.(1998). Clinical relevance of the distinction between alcohol dependence with and without a physiological component. American Journal of Psychiatry, 155, 733–740.
- Schulenberg, J., O’Malley, P. M., Bachman, J. G., Wadsworth, K. N., & Johnston, L. D. (1996). Getting drunk and growing up: Trajectories of frequent binge drinking during the transition to young adulthood. Journal of Studies on Alcohol, 57, 289–304.
- Searles, J. S. (1988). The role of genetics in the pathogenesis of alcoholism. Journal of Abnormal Psychology, 97, 153–167.
- (1942). Epistle LXXXIII: On drunkenness—Classics of the alcohol literature. Quarterly Journal of Studies on Alcohol, 3, 302–307.
- Shaffer, H., Hall, M., & Bilt, J. (1999). Estimating the prevalence of disordered gambling behavior in the United States and Canada: A research synthesis. American Journal of Public Health, 89, 1369–1376.
- Sharpe, L., Tarrier, N., Schotte, D., & Spence, S. (1995). The role of autonomic arousal in problem gambling. Addiction, 90, 1529– 1540.
- Sher, K. J. (1987). Stress response dampening. In H. T. Blane & K. E. Leonard (Eds.), Psychological theories of drinking and alcoholism (pp. 227–271). New York: Guilford Press.
- Sher, K. J. (Ed.). (1991). Children of alcoholics: A critical appraisal of theory and research. Chicago: University of Chicago Press.
- Sher, K. J. (1994). There are two types of alcoholism researchers: Those who believe in two types of alcoholism and those who don’t. Addiction, 89, 1061–1064.
- Sher, K. J., Bartholow, B. D., & Wood, M. D. (2000). Personality and substance use disorders: A prospective study. Journal of Consulting and Clinical Psychology, 68, 818–829.
- Sher, K. J., Bylund, D. B., Walitzer, K. S., Hartmann, J., & RayPrenger, C. (1994). Platelet MAO activity: Personality, substance use, and the stress-response-dampening effect of alcohol. Experimental and Clinical Psychopharmacology, 2, 53–81.
- Sher, K. J., & Gotham, H. (1999). Pathological alcohol involvement: A developmental disorder of young adulthood. Development and Psychopathology, 11, 933–956.
- Sher, K. J., & Trull, T. (1994). Personality and disinhibitory psychopathology: Alcoholism and antisocial personality disorder. Journal of Abnormal Psychology, 103, 92–102.
- Sher, K. J., Trull, T. J., Bartholow, B., & Vieth, A. (1999). Personality and alcoholism: Issues, methods, and etiological processes. In H. Blane & K. Leonard (Eds.), Psychological theories of drinking and alcoholism (2nd ed., pp. 55–105). New York: Plenum Press.
- Sieber, M. F. (1981). Personality scores and licit and illicit substance abuse. Personality and Individual Differences, 2, 235–241.
- Siegel, S., & Allan, L. G. (1998). Learning and homeostasis: Drug addiction and the McCollough effect. Psychological Bulletin, 124, 230–239.
- Siegel, S., Baptista, M. A., Kim, J. A., McDonald, R. V., & Weise-Kelly, L. (2000). Pavlovian psychopharmacology: The associative basis of tolerance. Experimental & Clinical Psychopharmacology, 8, 276–293.
- Sjoberg, L. (1969). Alcohol and gambling. Psychopharmacologia, 14, 284–298.
- Skinner, H. A. (1981). Primary syndromes of alcohol abuse: Their measurement and correlates. British Journal of Addiction, 76, 63–76.
- Slutske, W. S., Eisen, S., True, W., Lyons, M., Goldberg, J., & Tsuang, M. (2000). Common genetic vulnerability for pathological gambling and alcohol dependence in men. Archives of General Psychiatry, 57, 666–673.
- Slutske, W. S., Eisen, S., Xian, H., True, W., Lyons, M., Goldberg, J., & Tsuang, M. (2001). A twin study of the association between pathologicalgamblingandantisocialpersonalitydisorder.Journal of Abnormal Psychology, 110, 297–308.
- Slutske,W.S.,Heath,A.C.,Dinwiddie,S.,Madden,P.A.F.,Bucholz, K. K., Dunne, M., Statham, D., & Martin, N. (1998). Common genetic risk factors for conduct disorder and alcohol dependence. Journal ofAbnormal Psychology, 107, 363–374.
- Slutske, W. S., Heath, A. C., Madden, P. A. F., Bucholz, K. K., Statham, D. J., & Martin, N. G. (2002). Personality and the genetic risk for alcohol dependence. Journal of Abnormal Psychology, 111, 124–133.
- Smart, R. G., & Ferris, J. (1996). Alcohol, drugs and gambling in the Ontario adult population, 1994. Canadian Journal of Psychiatry, 41, 36–45.
- Smith, G. T., Goldman, M. S., Greenbaum, P. E., & Christiansen, B. A. (1995). Expectancy for social facilitation from drinking: The divergent paths of high-expectancy and low-expectancy adolescents. Journal of Abnormal Psychology, 104, 32–40.
- Solomon, R. L., & Corbit, J. D. (1974). An opponent-process theory of motivation: I. Temporal dynamics of affect. Psychological Review, 81, 119–145.
- Sproston, K., Erens, B., & Orford, J. (2000). Gambling behaviour in Britain: Results from the British Gambling Prevalence Survey. London: National Centre for Social Research.
- Spunt, B., Dupont, I., Lesieur, H., Liberty, H. J., & Hunt, D. (1998). Pathological gambling and substance misuse: Areview of the literature. Substance Use & Misuse, 33, 2535–2560.
- Stacy, A. W., & Newcomb, M. D. (1998). Memory association and personality as predictors of alcohol use: Mediation and moderator effects. Experimental & Clinical Psychopharmacology, 6, 280–291.
- Steel, Z., & Blaszczynski, A. (1998). Impulsivity, personality disorders and pathological gambling severity. Addiction, 93, 895–905.
- Steele, C. M. (1986). What happens when you drink too much? Psychology Today, 48–52.
- Steele, C. M., & Josephs, R. A. (1990). Alcohol myopia: Its prized and dangerous effects. American Psychologist, 45, 921–933.
- Stinchfield, R. (2000). Gambling and correlates of gambling among Minnesota public school students. Journal of Gambling Studies, 16, 153–173.
- Stinchfield, R., Cassuto, N., Winters, K., & Latimer, W. (1997). Prevalence of gambling among Minnesota public school students in 1992 and 1995. Journal of Gambling Studies, 13, 25–48.
- Stinchfield, R., & Winters, K. C. (1998). Gambling and problem gambling among youths. The Annals of the American Academy of Political and Social Science, 556, 172–185.
- Stritzke, W. G. K., Lang, A. R., & Patrick, C. J. (1996). Beyond stress and arousal: A reconceptualization of alcohol-emotion relations with respect to psychophysiological methods. Psychological Bulletin, 120, 376–395.
- Stritzke, W. G., Patrick, C. J., & Lang, A. R. (1995). Alcohol and human emotion: A multidimensional analysis incorporating startle-probe methodology. Journal of Abnormal Psychology, 104, 114–122.
- Stuss, D., & Benson, D. (1985). The frontal lobes. New York: Raven.
- Svanum, S. (1986). Alcohol-related problems and dependence: An elaboration and integration. International Journal of the Addictions, 21, 539–558.
- Tarter, R. E. (1988). Are there inherited behavioral traits that predispose to substance abuse? Journal of Consulting & Clinical Psychology, 56, 189–196.
- Toneatto, T. (1999). Cognitive psychopathology of problem gambling. Substance Use and Misuse, 34, 1593–1604.
- True, W. R., Xian, H., Scherrer, J. F., Madden, P. A. F., Bucholz, K., Heath, A. C., Eisen, S. A., Lyons, M. J., Goldberg, J., & Tsuang, M. (1999). Common genetic vulnerability for nicotine and alcohol dependence in men. Archives of General Psychiatry, 56, 655–661.
- Tsuang, M., Lyons, M., Eisen, S., Goldberg, J., True, W., Lin, N., Meyer, J., Toomey, R., Faraone, S., & Eaves, L. (1996). Genetic influences on DSM-III-R drug abuse and dependence: Astudy of 3,372 twin pairs. American Journal of Medical Genetics, 67, 473–477.
- Tsuang, M. T., Lyons, M. J., Harley, R. M., Xian, H., Eisen, S., Goldberg, J., True, W. R., & Faraone, S. V. (1999). Genetic and environmental influences on transitions in drug use. Behavior Genetics, 29, 473–479.
- Tsuang, M. T., Lyons, M. J., Meyer, J. M., Doyle, T., Eisen, S. A., Goldberg, J., True, W., Lin, N., Toomey, R., & Eaves, L. (1998). Co-occurrence of abuse of different drugs in men: The role of drug-specific and shared vulnerabilities. Archives of General Psychiatry, 55, 967–972.
- Vaillant, G. E., & Milofsky, E. S. (1982). The etiology of alcoholism: A prospective viewpoint. American Psychologist, 37, 494–503.
- Vitaro, F., Arsenault, L., & Tremblay, R. E. (1997). Dispositional predictors of problem gambling in male adolescents. American Journal of Psychiatry, 154, 1769–1770.
- Vitaro, F., Arsenault, L., & Tremblay, R. E. (1999). Impulsivity predicts problem gambling in low SES adolescent males. Addiction, 94, 565–575.
- Vitaro, F., Ladouceur, R., & Bujold, A. (1996). Predictive and concurrent correlates of gambling in early adolescent boys. Journal of Early Adolescence, 16, 211–228.
- Volberg, R. A., & Abbott, M. W. (1997). Gambling and problem gambling among indigenous peoples. Substance Use & Misuse, 32, 1525–1538.
- Volberg, R. A., & Banks, S. M. (1994). A new approach to understanding gambling and problem gambling in the general population. Paper presented at the Ninth International Conference on Gambling and Risk Taking, Las Vegas, NV.
- Volberg, R. A., & Steadman, H. J. (1988). Refining prevalence estimates of pathological gambling. American Journal of Psychiatry, 145, 502–505.
- Walker, M. (1992). Psychology of gambling. Woburn, MA: Butterworth-Heinemann.
- Wallisch, L. (1996). Gambling in Texas: 1995 surveys of adult and adolescent gambling behavior. Austin: Texas Commission on Alcohol and Drug Abuse.
- Warner, L., Kessler, R., Hughes, M., Anthony, J., & Nelson, C. (1995). Prevalence and correlates of drug use and dependence in the United States. Archives of General Psychiatry, 52, 219–229.
- Welte, J., Barnes, G., Wieczorek, W., Tidwell, M., & Parker, J. (2000). Alcohol dependence and pathological gambling: Comorbidity and comparative epidemiology in the U.S. New York: Research Institute on Addictions, and Center for Health and Social Research, Buffalo State College.
- West, D. J., & Farrington, D. P. (1973). Who becomes delinquent? London: Heinemann.
- White, J. L., Moffitt, T. E., Avshalom, C., Bartush, D. J., Needles, D. J., & Stouthamer-Loeber, M. (1994). Measuring impulsivity and examining its relationship to delinquency. Journal of Abnormal Psychology, 103, 192–205.
- Widiger, T. A. (1997). Mental disorders as discrete clinical conditions: Dimensional versus categorical classification. In S. M. Turner & M. Hersen (Eds), Adult psychopathology and diagnosis (3rd ed.). New York: Wiley.
- Windle, M., & Davies, P. T. (1999). Depression and heavy alcohol use among adolescents: Concurrent and prospective relations. Development & Psychopathology, 11, 823–844.
- Winters, K. C., Stinchfield, R., Botzet, A., & Anderson, N. (2001). Prospective studies of youth gambling behaviors. Unpublished manuscript.
- Winters, K. C., Stinchfield, R., & Fulkerson, J. (1993). Patterns and characteristics of adolescent gambling. Journal of Gambling Studies, 9, 371–386.
- Wise, R. A., & Bozarth, M. A. (1987). A psychomotor stimulant theory of addiction. Psychological Review, 94, 469–492.
- World Health Organization. (1967). Manual of the International Statistical Classification of Diseases, Injuries, and Causes of Death (8th ed.). Geneva, Switzerland: Author.
- Wray, I., & Dickerson, M. (1981). Cessation of high frequency gambling and “withdrawal” symptoms. British Journal of Addiction, 76, 401–405.
- Zucker, R. A. (1987). The four alcoholisms: A developmental account of the etiologic process. In P. C. Rivers (Ed.), Alcohol and addictive behaviors: Nebraska Symposium on Motivation (pp. 27–83). Lincoln: University of Nebraska Press.
- Zucker, R. A. (1995). Pathways to alcohol problems and alcoholism: A developmental account of the evidence for multiple alcoholisms and for contextual contributions to risk. In R. A. Zucker, G. M. Boyd, & J. Howard (Eds.), The development of alcohol problems: Exploring the biopsychosocial matrix of risk (NIAAA Research Monograph No. 26, pp. 255– 289). Rockville, MD: Department of Health and Human
- Zucker, R. A., Fitzgerald, H. E., & Moses, H. D. (1995). Emergence of alcohol problems and the several alcoholisms: A developmental perspective on etiologic theory and life course trajectory. In D. Cicchetti & D. J. Cohen (Eds.), Developmental psychopathology: Vol. 2. Risk, disorder, and adaptation. Wiley series on personality processes (pp. 677–711). New York: Wiley.
- Zucker, R. A., & Gomberg, E. S. L. (1986). Etiology of alcoholism reconsidered: The case for a biopsychosocial process. American Psychologist, 41,
- Zuckerman, M. (1991). Psychobiology of personality. New York: Cambridge University Press.
- Zuckerman, M. (1994). Behavioral expressions and biosocial bases of sensation seeking. NewYork: Cambridge University Press.
- Zuckerman,M.(1999).Vulnerabilitytopsychopathology:Abiosocial model. Washington, DC: American Psychological Association.
- Zuckerman, M., & Kuhlman, D. M. (2000). Personality and risktaking: Common biosocial factors. Journal of Personality, 68, 999–1029.
ORDER HIGH QUALITY CUSTOM PAPER

Always on-time

Plagiarism-Free

100% Confidentiality