Sample Clinical Psychology Research Paper. Browse other research paper examples and check the list of research paper topics for more inspiration. If you need a research paper written according to all the academic standards, you can always turn to our experienced writers for help. This is how your paper can get an A! Feel free to contact our custom research paper writing service for professional assistance. We offer high-quality assignments for reasonable rates.
Clinical psychology may be defined as “a scientific and professional field that seeks to increase our understanding of human behavior and to promote the effective functioning of individuals” (Reisman, 1991, p. 3). Clinicians share with other psychologists a valuing of truth and a commitment to its determination, which they believe is best done through scientific methods. However, they are also committed to being of help to people, who often present urgent problems that require immediate assistance. They emphasize the value and uniqueness of each individual and so strive to provide services to all populations. Thus, they have faced, and no doubt will continue to face, the dilemma of addressing insistent and pressing human needs with measuring instruments and methods of treatment whose validities are questioned by others, as well as by clinicians themselves.
Academic Writing, Editing, Proofreading, And Problem Solving Services
Get 10% OFF with 24START discount code
In this research paper, we are going to consider the history of clinical psychology through its various phases of development. We will view the field in the context of the changing milieu of attitudes and professional approaches that have characterized the area known as mental health. Throughout the relatively short history of the field, there have been differing views as to the roles of science and “art,” as well as both favorable climates (which we have titled zeitgeists) and resistance within the field. We shall also review the changing requisites for training and qualifying clinicians and treatment approaches and take a brief view of current and possible future developments.
Surprisingly, the history of clinical psychology is almost as long as the history of scientific psychology itself. Scientific psychology is often said to have begun when Wilhelm Wundt founded the first psychological laboratory at the University of Leipzig in 1879; clinical psychology can be said to have originated when Lightner Witmer, who earned his doctorate under Wundt established the first psychological clinic at the University of Pennsylvania in 1896 (Routh, 1996; Routh & DeRubeis, 1998; Witmer, 1897). Since at that time psychology itself was still in an early stage of gaining academic, scientific, and public acceptance, many psychologists had misgivings about the prudence of establishing an applied field of their discipline. In fact, almost a century later many clinicians believe such misgivings continue to remain detectable.
The early clinical psychologists thought of themselves as researchers, psychometricians (or measurers), and reeducators in the areas of individual differences, the ways in which people differ from one another, such as intelligence, personality, and abnormal behaviors. Yet it must also be pointed out and acknowledged that clinicians draw, more or less, from almost every area of psychology. So, recognizing the arbitrariness of what we are about, let us begin.
Lightner Witmer and the Founding of Clinical Psychology
Wundt and many of the early psychologists regarded psychology as the scientific study of consciousness. As empiricists, they believed that all that we know comes to us through our senses. Accordingly, they were interested in how we experience the world through our senses, in the acuity of our senses, and so on. When, in about 1884, Galton sought to measure intelligence, it seemed reasonable to do so by means of reaction time, sensory discrimination, height, weight, and other anthropometric indices. James McKeen Cattell, who was among the first Americans to receive a doctorate from Wundt, was most interested in Galton’s work and elaborated upon it.
Cattell (1890) introduced the term mental test and suggested administering a standardized battery of 10 tests, such as Least Noticeable Difference in Weight, Reaction-Time for Sound, and Judgment of Ten Seconds. Subsequently, in 1921, Cattell went on to found the Psychological Corporation, which has since become one of the world’s largest suppliers of psychological tests, but before he did that he had as one of his students at the University of Pennsylvania a fledgling psychologist by the name of Lightner Witmer (1867–1956).
Prior to studying psychology, Witmer was teaching English at Rugby Academy, a prep school in Philadelphia, where one of his pupils had an articulation problem. Witmer had been considering a career in law or business, but this youngster’s difficulties with speech aroused his interest. Upon investigating further, he concluded the problem derived from a head injury suffered at the age of 2 and speculated that with proper diagnosis and treatment, this youngster could have avoided years of frustration and embarrassment. That psychology might be of help to those who had such problems was a factor in leading Witmer to major in the new science.
After he received his doctorate in 1892,Witmer returned to the University of Pennsylvania and took over the psychology laboratory from Cattell, who left to assume a similar position at Columbia University. While teaching a course in psychology at Pennsylvania, Witmer was challenged by one of his students, Margaret Maguire, a teacher in the Philadelphia public schools, to use psychology to be of help to children with learning problems. Specifically, she asked Witmer to help a 14-year-old who seemed to be of normal intelligence yet was three grades retarded in spelling. Witmer put the adolescent through a diagnostic process and found a visual anomaly that was partially corrected by glasses. Then, by having the child tutored, some improvement was effected, though the situation was considerably more complex than originally presented (McReynolds, 1997; Witmer, 1907a).
Witmer was sufficiently encouraged by this success and sufficiently convinced that psychology could be helpful to persuade the university administration to back the creation of a psychology clinic in 1896. Later that year, at the American Psychological Association (APA) convention, he reported to his colleagues what he had done and urged them to do likewise. He spoke of a “clinical method,” which would educate students through demonstrations and contacts with those who required the services of psychologists. Thus, the psychological clinic would be an agency for instruction, original research, and service to the community (Reisman, 1991; Witmer, 1897).
The treatments Witmer practiced and taught were essentially pedagogical. In so doing, he carried on in the tradition of such pioneers as J. Rodriguez Pereira, who taught the deaf to speak; J. M. G. Itard, who attempted to educate and civilize Victor, the Wild Boy of Aveyron; and Edouard Seguin, who set up the first school to train those with mental retardation (Routh, del Barrio, & Carpentero, 1996). However, it should also be recognized that Witmer, in common with many clinicians today, believed that a broad range of problems indicated the need for remediation and training. To Witmer, a juvenile delinquent was deficient in moral training or proper conduct, and he thought of a child who might be regarded as psychotic today as developmentally arrested in a variety of behaviors that required correction.
In assessing the person, Witmer at first relied upon observation and whatever psychometric devices were available, which were then not very many. He also availed himself of the services of social workers, teachers, and any other professional who might be indicated, such as neurologists, optometrists, and physicians. A few years after Alfred Binet developed the first age scale for measuring children’s intelligence in France (Binet & Simon, 1905), Witmer incorporated a version of it into his clinical assessment procedures. Another important aspect of how Witmer viewed assessment was that he saw the attempted remediation of a problem as an opportunity to test his understanding of it. Thus, he regarded treatment as part of assessment and to be often decisive in determining the validity of one’s diagnosis.
About a decade after the founding of the clinic,Witmer appealed to Philadelphia philanthropist Mrs. J. Lewis (Mary L.) Crozer for funds to establish a clinical journal. By then, Witmer was offering courses and a training program in this new field of psychology and appeared to be successfully serving the community. She agreed to give him the money, and in 1907, a journal called The Psychological Clinic began publication. For the next 30 years, until it ceased publication in 1937, Witmer served as its editor, frequent contributor, occasional book reviewer, and gossip columnist. In its first issue, Witmer (1907b) wrote what is perhaps the most significant article in the history of clinical psychology (McReynolds, 1997).
Witmer called for the creation of the field of clinical psychology as an independent profession, though grounded in the science of psychology. While his experiences had been almost exclusively with children, he made it clear in the last paragraph of the article that clinical psychology could help others as well:
I would not have it thought that the method of clinical psychology is limited necessarily to mentally and morally retarded children. . . . The methods of clinical psychology are necessarily invoked wherever the status of an individual mind is determined by observation and experiment, and pedagogical treatment applied to effect a change, i.e., the development of such individual mind. Whether the subject be a child or an adult, the examination and treatment may be conducted and their results expressed in the terms of the clinical method. (Witmer, 1907b)
Witmer also recognized that clinical psychology encroached to some extent upon the field of psychiatry. However, he believed that given the proper training, the clinical psychologist could make contributions that were distinctive and valuable. Such training was being provided under Witmer’s direction in the psychological clinic and through formal graduate-level course work in developmental psychology, abnormal psychology, and mental and physical defects of school children.
By 1909, the staff of the psychological clinic consisted of Witmer as director, an assistant director, five trained PhDs as examiners, a social worker, and three assistant social workers. They were no longer alone. The Iowa Psychological Clinic was founded in 1913 by Carl Seashore and R. L. Sylvester (Routh, 1984), and a psychological clinic was also established at Clark University in 1913. Moreover, there were courses in clinical psychology and there would soon be clinics at the University of Minnesota and the University of Washington (Reisman, 1991).
Also by 1909, Witmer was urging a broader goal for clinicians and “orthogenics” as a new designation for the field. Orthogenics included all that is now meant by the terms primary, secondary, and tertiary prevention, as well as the human potential movement. This was to be a profession concerned with human development, both of the individual and the species. Whatever was determined to impede or distort development, including social conditions and public policies that might be damaging, was grist for the clinician’s mill and should be identified and remedied. With regard to the nutritional, intellectual, and emotional deprivations of poor children, Witmer (1909–1910) stated, “The problem calls for preventive social action. . . . We should offer the slum parent something better than a choice between race suicide and child murder.”
He began to subtitle The Psychological Clinic as A Journal of Orthogenics, and each issue thereafter carried that subtitle and a definition of orthogenics: “While orthogenics concerns itself primarily with the causes and treatment of retardation and deviation, it is by definition the science of normal development, and comprehends within its scope all the conditions which facilitate, conserve, or obstruct the normal development of mind and body” (Witmer, 1925). Obviously, in view of the title of this research paper not too many people warmed up to orthogenics as a new designation, but Witmer’s vision for the scope of the field he began has gained in acceptance over the years.
A Scientific Art?
Scientific psychiatry is probably best regarded as originating around the nineteenth century, though like scientific psychology it can trace its origins back over 2,000 years to the philosophers and medical practitioners of ancient Greece. Hippocrates spoke of mania, melancholia, phrenitis, hysteria, and paranoia and thought of these as medical disorders, probably brought about by an excess of one type or another of humor, or bodily fluid (Routh, 1998). By and large, however, he recommended that patients with mental disorders be treated with kindness, soothing music, and rest. The Roman physician Galen (A.D. 129–198), promoted the view that the etiology of specific disorders lay with excess humors, such as black bile, yellow bile, blood, and phlegm, which led to the treatment of the mentally ill with purges, vomits, bleeding, and expectorants; these were the treatments widely used in Western societies to the end of the eighteenth century.
During the eighteenth century, there emerged on several fronts a different way of looking at people. The philosopher Jean-Jacques Rousseau (1712–1778) argued that people are naturally good but that they are corrupted by their society. If allowed to develop naturally, or freely to experience the world and the consequences of their behaviors, a natural goodness or nobility would be expressed. Rousseau argued it was the artificialities of the social order that drove people to despair and that a simple life, close to nature, was best. Clearly Rousseau’s influence can be seen today in natural remedies and holistic medicine.
Moral treatment, treating the mentally disturbed with kindness and respect rather than with physical force, restraints, or harsh medications, began to be practiced toward the end of the eighteenth century. In France, Philippe Pinel (1745–1826), called the father of scientific psychiatry because he introduced case histories and maintained records for his patients and because he tried to develop a nosology, advocated humane treatment for the mentally ill.Afamous picture of Pinel “striking off the chains” of an unfortunate patient is depicted in many books on abnormal psychology and psychiatry. Contrary to legend, Pinel was not the first to unchain the insane.
In England, a Quaker tea merchant, William Tuke (1732– 1822), established the York Retreat, where kindness and decency in a rural setting were provided for the disturbed. In Italy, Vincinzo Chiarugi opposed restraints and cruel measures, and in the United States, Eli Todd urged physicians to practice moral treatment and established the Retreat in Hartford. Social reformers, such as Dorothea Dix, advocated the building of mental hospitals to provide humane care for the mentally ill, and during the nineteenth century more than 30 state institutions, as well as asylums in Europe, were erected as a direct result of her efforts.
By the middle of the nineteenth century, moral treatment was being employed at a number of mental hospitals amid enthusiastic reports of high recovery and discharge rates. During this same period, the profession of psychiatry was also growing. The Association of Medical Superintendents of asylums for the insane, the precursor of the American Psychiatric Association, was founded in 1844, about the same time as similar organizations were founded in France and England. Its major publication was the American Journal of Insanity, which became the American Journal of Psychiatry, now in 2002 is in its 159th consecutive year of publication.
Breakthroughs were occurring in the scientific determination of the etiologies of a variety of mental disorders. In 1826, the French physician Antoine L. Bayle found an association between general paresis of the insane, a psychotic condition that led to dementia and paralysis, and chronic inflammation of the meninges. Richard von Krafft-Ebing’s experiments demonstrated that paresis was caused by syphilis. Sergei Korsakov reported the harmful effects of chronic alcoholism on brain functioning. Karl Wernicke studied the effects of lesions in different areas of the brain and different forms of language disturbances or aphasias. It seemed to Emil Kraepelin, and to many other psychiatrists, that what was needed was the determination of the syndromes of specific disorders, research into their etiologies and their natural courses, and the development of their specific treatments. For a detailed review of this period, see Alexander and Selesnik’s History of Psychiatry (1966).
Therefore, toward the end of the nineteenth century, the attitude toward moral treatment changed. Mental hospitals began to be seen mainly as custodial institutions for the mentally ill, who required further scientific study until appropriate treatments could be determined. It was suggested that the improvement rates for moral treatment had not been scientifically determined and were probably grossly exaggerated. Lower rates of improvement with moral treatment were reported, and its defenders attributed these to a more intransigent and difficult patient population and to a newer generation of psychiatrists who lacked the zeal and conviction of earlier practitioners (Levine, 1981). Sound familiar? Additional research, it was generally agreed, for this and other questions, would soon settle matters.
The major neurosis at this time was hysteria, whose symptoms had an annoying similarity to those of many neurological disorders. Jean-Martin Charcot, a leading neurologist of his day, used a cast of hysterics who had been previously hypnotized to demonstrate to his colleagues that all the various symptoms of hysteria—paralyses, crying spells, anesthesias—could be produced and modified under hypnosis. Charcot concluded, incorrectly, that there was an intimate relationship between hysteria and hypnosis and thus those who could be hypnotized either had hysteria or were predisposed to develop this neurosis (Goetz, Bonduelle, & Gelfand, 1995). An interested spectator at some of Charcot’s demonstrations in 1885 was the Viennese neurologist Sigmund Freud (1856–1939).
Freud had gone to Paris to learn the latest thinking about the treatment of hysteria. An older colleague of Freud’s, Josef Breuer, had become involved in an interesting case, in which the patient suggested talking about problems. This talking seemed to be of help, and Charcot’s hypnotic demonstrations supported Freud in his belief that whatever the etiology of hysteria, the symptoms could be treated and reduced by verbal means. By 1892, Freud abandoned hypnosis in favor of a “concentration” technique, in which the patient was directed to try to recall all memories in connection with a symptom. By 1895, Freud was talking about “psychical analysis,” or “psychoanalysis,” and his relationship with Breuer was close to an end (Breuer & Freud, 1895/1955; Gay, 1988).
Within the first decade of the twentieth century, Freud was rapidly developing psychoanalysis as a theory of personality, which he regarded as his contribution to psychology; as a method of treatment, which he believed was of limited use because of its expense, duration, and the few analysts available; and as a way of doing research. He had achieved international recognition and had adherents throughout Europe and in the United States. In 1909, the eminent developmental psychologist G. Stanley Hall invited Freud to come to Clark University to address a gathering of American psychologists who would be participating in the celebration of the school’s 20th anniversary. One of the members of that audience was William James.
An Artistic Science?
William James (1842–1910), like many of the other early psychologists such as Wundt, had originally trained to be a physician. For 12 years, he labored to produce a psychology text that would serve to help him appraise the field, and in 1890 his magnum opus, Principles of Psychology, was published. It quickly became a classic, and despite the early stage of development of scientific psychology when it was written, much within it would be of interest to clinicians today. There was a chapter on the unconscious mind and the evidence for its existence: that ideas or thoughts that are seemingly forgotten must be existing somewhere if they can be recalled; sleepwalkers who have no memory for what they did; our ability to sense the boundaries of our beds while asleep and to awaken close to a desired time; posthypnotic suggestions and movements carried out automatically by hysterics. In contrast, the unconscious mind as it would soon be conceived by Freud affected human functioning all through the day and night, in dreams as well as in neurotic symptoms, in daily accidents and thoughts and memory lapses and decisions.
There was a lengthy discussion of the Self, which in James’s view was the sum total of all that the person owned: a Material Self consisting of the person’s clothing, property, body, and family; a Social Self composed of the many roles people played in different kinds of interactions; and a Spiritual Self, consisting of the person’s conscience and will, values, and psychological faculties. And there was often conflict between these different aspects of self, which had to be resolved by simply deciding what should be given expression and what should be suppressed. According to James, it was simply impossible to give expression to all aspects of oneself.
James had a much more rational view of human behavior than Freud. In his own life, prior to becoming a psychologist, James had overcome feelings of depression by sheer strength of resolve. He asserted that people could control their emotions if they determined to do it and by exhibiting characteristics of the feeling they wished to have. In other words, to be happy, smile and act happy, and you will begin to experience happiness . . . or as Shakespeare eloquently put it in Henry V in exhorting troops to do battle bravely: “Stiffen the sinews, summon up the blood, Disguise fair nature with hard-favor’d rage” (act 3, scene 1).
An equally straightforward approach was recommended to build good habits and break bad ones. Just go to it, and allow no exceptions to the doing of the habit you wish to achieve and immediately stop doing the habit you want to break. For James, it made no sense to try to gradually wean yourself from doing what you supposedly wanted to stop doing.
Similarly, James argued in his discussion of the self that people had it in their power to raise their self-esteem. He reasoned that our feelings about ourselves are determined by our accomplishments divided by our aspirations. If we wished to feel better about ourselves, we could raise our self-esteem by achieving more of our goals or—and this was the easier course—by lowering our aspirations and pretensions.
These practical suggestions made sense to James, who was shortly to become a leading proponent of pragmatism, a philosophical system that stresses that the value or merit of a truth or undertaking lies in its practical consequences. However, in the opinion of those who favored psychology as a “pure” science, these practical matters were totally extraneous to the field. James was not so sure psychology was headed in the right direction, and in 1907 he became a professor of philosophy. Within six years, a movement called behaviorism was launched against the prevailing psychology of Wundt and introspection.
It was in 1913 that John B. Watson proclaimed psychology to be “a purely objective experimental branch of natural science. Its theoretical goal is the prediction and control of behavior.” Using as his model the reflex, Watson argued that all psychology needed to be concerned about were stimuli and responses: given the stimuli, to determine the responses; given the responses, to discover the stimuli. Research using introspection was best avoided, and psychologists should endeavor to put their findings to practical use (Watson, 1913). In 1915, Watson became president of the American Psychological Association (APA), while the numbers of psychologists who regarded themselves as behaviorists grew with each year. Their focus was not on sensation or perception but on learning, and they were not averse to seeing the process of learning in all areas of human functioning.
A Sustaining Zeitgeist
Another way of looking at the fact that Witmer was successful when he approached his university looking for funds for a psychology clinic and when he contacted a philanthropist for money to start a journal in clinical psychology is to say the zeitgeist was favorable. We have already considered a number of events that during the eighteenth and nineteenth centuries prepared the way for the development of this field, and here we shall note others that promoted its advance during the early part of the twentieth century.
However, it would be incorrect to suggest the going was smooth and easy. The APA, founded in 1892 with 31 members, had only about 300 by 1917; its purpose was solely to promote the advance of psychology as a science, and it was reluctant to become involved in what many of its members considered extraneous issues, such as what the qualifications of a psychological examiner were and whether clinical psychologists should be supported when their expertise was challenged by psychiatrists. Not surprisingly, while there may have been a need for the services of clinical psychologists in the society at large, at this stage in the development of the field there was little demand.
Accordingly, the training of clinicians was haphazard and withoutanyuniformity.Afewuniversitiesprovidededucation for clinicians, but most professionals had to take what courses they could in college and seek further training on the job in mental hospitals and clinics. In the former setting, they thought of themselves as primarily researchers in abnormal functioning; in the latter, they regarded themselves as mainly psychometricians and educators with children. (It should be remembered that the first individually administered intelligencescalestandardizedonadults,theWechsler-Bellevue,did not become available until 1939.) With these sobering qualifications stated, let us note some of the positive influences.
Morton Prince (1854–1929), a neurologist at Tufts Medical College, founded the Journal of Abnormal Psychology in 1906 and served as its editor for many years. He was particularly interested in hysteria and multiple personalities and thought that the same processes that govern learning can be used to explain abnormal behaviors. Neuroses, for example, were often perversions of associations, because neurotics often had difficulties in recalling the past. Psychotherapies, he concluded, are actually different ways of educating people to associate differently and thus adjust better to their environments (Prince, 1909–1910). While working in Boston, Prince met with a congenial circle of physicians and psychologists, including Boris Sidis and William James, to discuss psychopathology and its treatment. He was sympathetic to psychoanalysis and through his journal helped to make it known. In 1927, he founded the Harvard Psychological Clinic, and by making it a unit of the Department of Psychology, he sought to ensure that the study of personality and psychopathology was regarded as part of psychology rather than psychiatry.
William James received a visit in 1906 from a former mental patient who had written a book about his experiences in treatment. The book was titled A Mind That Found Itself, and its author was Clifford Beers (1908). James read the manuscript and wrote a letter of endorsement, which became part of the book’s introduction and which served to bring others to Beers’s support. Clifford Beers (1876–1943) wanted to establish a movement that would make the public aware of mental illness and willing to provide for its alleviation and treatment. This became known as the mental hygiene movement, and Beers founded the first of its many societies in Connecticut in 1908.
That same year a prominent social worker, Julia Lathrop, met with a psychiatrist, William Healy (1869–1963), in Chicago to consider what new approaches to juvenile delinquency might be of help. At that time, judges disposed of delinquents with nothing more than the results of a physical examination to guide them. Certainly their decisions could be better informed, and as a first step, research might be conducted to determine the causes of delinquency. Healy went off to get ideas by meeting with James and other psychologists and by visiting the clinics of Witmer and Goddard. Influenced by the favorable recommendation of William James, Julia Lathrop asked Healy to be the director of the new clinic, which, when it opened in 1909, was called the Juvenile Psychopathic Institute and today is known as the Institute for Juvenile Research. Its original staff consisted of Healy; a clinical psychologist, Grace Fernald (who later moved to California, where she developed innovative practices for remediating reading disorders in children and where a school was named in her honor by UCLA); and a secretary. Many consider it the first child-guidance clinic in the world.
A number of judges visited Healy’s clinic, with the idea in mind to assess whether a similar operation could work with their courts. During the summers of 1912 and 1913, Healy taught a course at Harvard describing his work, and in 1917 he and Augusta Bronner, a clinical psychologist whom he married, moved to Boston to establish the Judge Baker Guidance Clinic. The focus of these clinics affiliated with the courts was to evaluate children by means of psychological tests, mainly intelligence tests, and other means in order to make recommendations to juvenile-court judges regarding the disposition of their cases. Healy, it should be added, thought of himself not only as a psychiatrist but also as a clinical psychologist; he developed two performance measures of intelligence, one of which, the Healy Picture Completion Test, was quite popular in its day.
During World War I, Robert Yerkes (1876–1956), a comparative psychologist at Yale (who later had primate laboratories, now at Emory University, named in his honor) and also a clinician who made the Binet into a point scale (Yerkes, Bridges, & Hardwick, 1915), chaired a committee of psychologists that was asked to develop a group-administered scale of intelligence for the army. This committee produced the Army Alpha, a verbal scale; the Army Beta, which was nonverbal and intended for those who could not read English; and the Personal Data Sheet, a neurotic inventory designed by Robert Woodworth that was one of the earliest personality questionnaires (Yerkes, 1919). Almost two million men were assessed with the Army Alpha and Beta tests, and Yerkes believed the prestige of psychology had been enhanced by its contributions to the war effort.
On December 28, 1917, an organization known as the American Association of Clinical Psychologists (AACP) was founded by J. E. Wallin, Leta Hollingworth, Rudolf Pintner, and three others. Aside from conviviality, the AACP came into being because clinicians wanted a group that would be forceful in addressing their concerns, such as mental tests being administered by nonqualified examiners and clinicians gaining legal recognition as experts in the determination of mental retardation and psychopathology.
Robert Yerkes, the president of the APA at the time and also a member of AACP, negotiated with the dissidents and convinced them their interests would be best served through the APA. Accordingly the AACP went out of existence in 1919 and became the Clinical Section of the APA, the first of what were to become the many divisions of that organization. About the only activity of the AACP during its brief life was to sponsor a symposium at the 1918 APA convention. The room was so jammed with people that it was not possible to present this program, but the papers were published the next year in the Journal of Applied Psychology. David Mitchell is regarded as the first to earn his living through private practice; he obtained his PhD from the University of Pennsylvania (Meltzer, 1966; Mitchell, 1919, 1931) and reported that his treatment approach involved strengthening and eliminating habits.
The number of child-guidance clinics began to grow during the 1920s with the support of the Commonwealth Fund, established by the Harkness family which also funded the National Committee for Mental Hygiene to seek the causes and prevention of juvenile delinquency. These clinics, usually staffed by psychiatrists, clinical psychologists, and social workers and concerned with the diagnosis and treatment of child problems of all sorts, from infancy through adolescence, served as additional sources of employment for clinicians. By 1930, there were about 500 clinics in the United States offering psychiatric services, of which about 125 were child guidance; by 1936, there were 676 psychiatric clinics and 87 psycho-educational clinics, the latter mostly affiliated with colleges and directed by psychologists.
In 1924, the psychiatrist Karl Menninger met with a group of colleagues at the Institute for Juvenile Research to form the American Orthopsychiatric Association. Its first president was William Healy. Although voting membership in the group was initially restricted to psychiatrists, this restriction was dropped within 2 years. Among the clinical psychologists in this organization were Lightner Witmer, Augusta Bronner, Shepherd Franz (one of the first clinical neuropsychologists), Henry Goddard, and Edgar Doll (1920). The association soon began publication of a journal, The American Journal of Orthopsychiatry, which still focuses on interdisciplinary research and advocacy regarding the mental health problems of children and families.
John B. Watson returned from service in World War I and set about to determine what unconditioned stimuli produce what unconditioned emotional responses in infants. He was particularly interested in fear and was aware that Freud (1909/1959) had presented a case of a boy who had a phobia of horses, which through analysis was discovered to be a fear of his father.Watson found that loud noises and sudden loss of support elicit fear in infants and that by pairing a loud noise with a white rat, a fear response could not only be conditioned to the rodent but could be generalized to other furry objects (Watson & Raynor, 1920). Unfortunately the infant, Albert, became unavailable for Watson to extinguish the response. However, Mary Cover Jones (1924), subsequently a prominent developmental psychologist, did demonstrate that a child’s fear of rabbits could be reconditioned by bringing a rabbit closer and closer while the boy ate lunch. Here was evidence, Watson believed, to suggest that some irrational fears in children might be brought about and treated through conditioning and without any need to invoke unconscious conflicts.
Nevertheless, psychoanalytic concepts were winning the day. They were gaining in popularity among mental health professionals. Morton Prince was moved to remark: “Freudian psychology had flooded the field like a full rising tide and the rest of us were left submerged like clams in the sands at low water” (quoted by Hale, 1971, p. 434). In 1924, William Alanson White, then president of the American Psychiatric Association, urged psychiatrists to incorporate psychoanalytic concepts into their thinking and to use analysis to gain fresh insights into mental illness. Psychologists were impressed not only by Freud’s ideas but by the ideas of those who disagreed with Freud, such as Alfred Adler and his notions about the significance of birth order and the inferiority complex, and Carl Jung and his introvert/extrovert personality types. Moreover, there were new tests of personality, like the Rorschach and the TAT, which relied upon an appreciation and an understanding of unconscious functioning to be administered and interpreted. Further, there began to be a new way of looking at neurosis, as illustrated in the analyst Karen Horney’s (1937) book, The Neurotic Personality of Our Time. Neuroses, Horney argued, are brought about by disturbances in interpersonal relations, and their symptoms are determined by their culture and period. The conditions that existed for Freud differ from those that are current. Were we to analyze our culture, we would find different kinds of confusion and conflict from those of turn-of-the-century Vienna. Therefore, we see fewer hysterics and more neuroses of character, whose symptoms involve difficulties in relating to people effectively. Similar ideas were being expressed by Franz Alexander, Erich Fromm, and Wilhelm Reich (see Munroe, 1955).
Organizational Struggles and Training Models
Clinicians persisted in trying to get the APA to address their professional concerns, but theAPAstill wavered. In 1931, the Clinical Psychology section of the APA tried to set standards for a training program in clinical psychology. A committee was appointed and within 4 years issued its report: Clinical psychology was defined as “that art and technology which deals with the adjustment problems of human beings”; it required of its practitioners the PhD and a year of supervised experience; an MAand a year’s experience would qualify one to be an assistant psychologist (Report of Committee, 1935). Then considering its task finished, this committee disbanded.
Evidently tiring of frustration, in 1937 the Clinical Psychology section of the APA dissolved itself and became instead a section of a new organization known as the American Association of Applied Psychology (AAAP). This clinical section had 229 members at its founding (Routh, 1994, 1997). When the clinical section had first affiliated with APA, part of the agreement had been that the section would be allowed to continue its focus on the professional as well as the scientific aspects of the field. As time went on, the APA did not live up to this agreement, and the section’s annual meeting became merely a place to read scientific papers. Also, the APA had agreed to set up a system for certifying “consulting psychologists” as qualified to offer their services to the public. Only 25 persons were ever so certified before the system was discontinued in 1927. The AAAP also incorporated the Association of Consulting Psychologists, which had been founded in 1931, and began publishing its Journal of Consulting Psychology. (It continues to enjoy a fine reputation as a premier publication for clincians’research as the Journal of Consulting and Clinical Psychology.)
With all this unrest and with all the excitement psychoanalysis and its offshoots were generating in psychiatry and in the culture, it is small wonder that clinicians began to want to become more involved in treatment and saw their roles as researchers, psychometricians, and educators to be somewhat lacking in prestige, status, and pizzazz. Could treating enuresis by a bell and pad apparatus (Mowrer & Mowrer, 1938) compare in sophistication with determining why a child unconsciously resisted the toilet-training efforts of parents? World events would shortly push that question a bit to the side and afford clinicians an unprecedented opportunity for the growth of their profession. But before we consider the momentous events that happened—U.S. participation in the Second World War from 1941 to 1945—let us take a closer look at the training of clinicians in the prewar period.
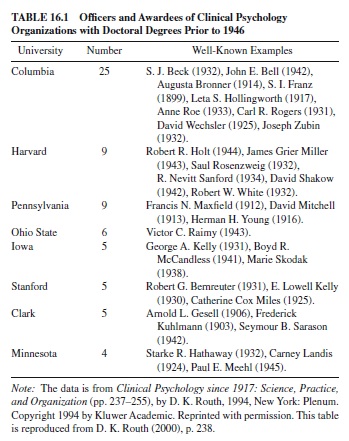
If we examine those clinical psychologists who achieved eminence in the field, as indicated by recognition from their colleagues through awards or election to office in professional organizations, we find that many of them earned their doctorates from only a handful of schools. A list of schools whose graduates became prominent clinical psychologists is shown in Table 16.1. As this table shows, the University of Pennsylvania, Columbia, and Harvard had large numbers of successful graduates, with Columbia alone accounting for more than twice as many as any other school (Routh, 2000). Yet even at many of these universities, such as Harvard, there was no prescribed course work or training to become a clinical psychologist. David Shakow, for example, took what relevant courses and training he could, which he described as a “do-it-yourself program” (Shakow, 1976), and his experiences were more the rule than the exception.
The internship is generally regarded as one of the most significant experiences in the training of clinicians (Doll, 1920). The Training School at Vineland, an institution for persons with mental retardation, is considered the first nonuniversity institution to offer an internship, beginning in 1908. Routh (2000) identified 26 psychology internships that were established before 1946. According to Morrow’s (1946) personal communication from William Healy, psychology interns would stay “for at least a year, the tenures sometimes overlapping for considerable periods. These students engaged in psychometric examinations and in research and attended all staff meetings” (p. 168). What is of significance about this description is that prior to 1946, training in psychotherapy for clinical psychologists was more the exception than the rule.
A Nurturing Zeitgeist
World War II represents a watershed in the history of clinical psychology. In its aftermath, clinical psychology received something it had not received before: enormous institutional support from the federal government, from universities, and from the APA for the training of clinical psychologists. In 1942, Robert Yerkes chaired a committee of the National Research Council, which sought to unite the AAAPand the APA by drafting a new constitution that would be acceptable to both groups. Such a constitution was drafted and provided for an APAdedicated “to advance psychology as a science and as a means of promoting human welfare.” Henceforth, the APA would be involved in professional and scientific issues, and a new journal, American Psychologist, would give coverage to both concerns. In 1944, the APA accepted the new constitution, the AAAP transferred its membership of about 600 psychologists to the APA, and the dues went up. American Psychologist began publication in 1946. The new APA had a divisional structure, in which psychologists with similar interests could affiliate. Division 12 was the division (now known as the Society) of Clinical Psychology, and it for a time became APA’s largest division.
Even before America’s entry into the war, oppressive dictatorships in Europe had brought about an influx of psychologists to the United States who did much to invigorate and enrich American psychology. Many of the leading Gestalt psychologists, such as Max Wertheimer, Wolfgang Kohler, Kurt Koffka, Kurt Lewin, and many lay analysts (that is, those without MD degrees), such as Erik Erikson, Erich Fromm, and Hanns Sachs, immigrated to this country. Many who were recognized psychoanalysts in Europe found their practices impeded by theAmerican PsychoanalyticAssociation, which had a long history of opposition to lay analysts, despite Freud’s precepts to the contrary (Freud, 1927).At training institutes under its aegis, the American Psychoanalytic Association would admit only physicians, unless a nonphysician first agreed to use his or her education only for purposes of research or self-enlightenment and not to train nonphysician colleagues in psychoanalysis. European psychologists such as Theodore Reik did not accept these restrictions. Instead, Reik founded his own psychoanalytic training institute in the United States, which welcomed psychologists and other mental health professionals.
As the war drew to a close, it was recognized that there were going to be enormous demands for clinical psychologists to provide their services to veterans. There were 16 million veterans of World War II and 4 million veterans of previous wars. The VeteransAdministration (VA) estimated it alone would need 4,700 clinical psychologists and vocational counselors, and there was nothing close to that number of clinicians. A joint APA and AAAP committee, with David Shakow as chairman, began meeting in 1944 to address the problem. That committee decided that rather than develop new professional schools, it would be better to use existing universities and programs.A4-year graduate course of instruction leading to the PhD degree was proposed: the first year to ground the student in psychology as a science, research methodology, and theory; clinical courses, practicums, and an internship would be in the second and third years; and the fourth year would involve finishing the doctoral dissertation.
All the planets and stars seemed to be in the proper alignment. The chief of the Division of Clinical Psychology and Neuropsychiatry at the VA was James G. Miller, who earned simultaneously both a PhD in psychology and an MD at Harvard; he recognized the value of clinical psychologists, supported their training in psychotherapy, and sought to give them equal status with psychiatrists (Hilgard, 1987). The APA endorsed the graduate program recommended by the committee and agreed to evaluate and monitor schools and training facilities to ensure they were meeting standards. Robert Felix, a psychiatrist who was the first director of the newly created National Institutes of Mental Health (NIMH), was also friendly toward psychology; in 1946, the NIMH began its program of training grants and was soon awarding over $200,000 a year to students in clinical psychology and making funds available for psychological research. Also in 1946, the APA published its first list of acceptable schools for graduate training in clinical psychology, realizing there was much more to be done in setting standards.
In 1947, Carl Rogers, as president of the APA, appointed David Shakow to chair yet another Committee on Training in Clinical Psychology (Shakow, 1965). This committee recommended that courses for clinicians should include psychotherapy and psychodynamics, with coursework in related areas—for example, anthropology, medicine, and sociology— germane to the particular student. These recommendations appeared to extend the duration of graduate education beyond the bounds of what was seemly, so in 1949 theAPAheld a conference in Boulder, Colorado, to discuss training policies in clinical psychology.
The Boulder Conference had 73 attendees, most of whom were intimately involved in the graduate education of clinicians. It was the first national meeting to consider standards for their doctoral training. Basically, the conference decided to endorse a solid grounding in science and practice, and this scientist-practitioner role for the clinical psychologist came to be called the Boulder model. (It reflected David Shakow’s own background, which included a lengthy research-clinical apprenticeship at Worcester State Hospital in Massachusetts, a personal psychoanalysis undertaken in part to prepare for research in that area, and a career dedicated largely to studies of motor performance and attentional deficits in schizophrenia, both before and after he became chief psychologist at NIMH.) Despite its endorsement of the scientist-practitioner model, the Boulder Conference also urged graduate schools to be flexible and innovative in their training (Benjamin & Baker, 2000; Raimy, 1950). Of most significance was that psychotherapy or treatment became an essential component in the training of the clinical psychologist.
Since it is rare to find unanimity about anything, not all clinicians welcomed this change in their profession. Hans Eysenck (1949), for one, spoke against it. He gave three reasons why it would be better for clinicians not to become therapists: Treatment is a medical problem; training in therapy reduces the time available for training in research and diagnosis; and becoming a psychotherapist biases the clinician from studying its effectiveness objectively. His comments, however, had little immediate impact, and most students of clinical psychology saw the learning of psychotherapy as the sine qua non of their graduate education.
While there was concern about standards and models, there was explosive growth in the profession. From a handful of universities offering graduate training in clinical psychology before the war, the number grew to 22 by 1947, 42 by 1949. Each of these programs reported it had far more applicants than it could accommodate. This interest in clinical psychology was spurred by a growing interest in psychological matters in the culture through movies, literature, newspaper accounts, art, self-help books, and so on. At the same time, clinical psychologists were beginning a national drive for legal recognition and protection of their field.
Within the states, legislators were being asked to enact licensing and certification laws for psychologists. A certification law restricts the use of the title “psychologist” by specifying the criteria that must be met by those who wish to use it. A licensing law restricts the performance of certain activities to members of a specific profession. Because some of the activities of clinicians overlap with some of the activities of other professions, the APA favored certification over licensing legislation. The first state to enact a certification law for psychologists was Connecticut in 1945; it restricted the title of psychologist to those who had a PhD and a year of professional experience. In 1946, Virginia enacted a certification law for clinical psychologists that required the PhD and 5 years of professional experience.
The passage of this legislation often encountered stiff resistance from the medical profession. Many psychiatrists, such as William Menninger, respected clinical psychologists and felt they had a major contribution to give to the psychiatric team through their diagnostic testing and research. According to this view, clinical psychologists could even do psychotherapy under medical supervision, but they should be barred from the private practice of treatment because they lacked the keen sense of responsibility felt by physicians for their patients (Menninger, 1950).
Recognizing that certification or licensure by the states would be a difficult, lengthy process, it was decided in 1946 to establish a kind of certification by the profession, and thus was created the American Board of Examiners in Professional Psychology (ABEPP). The board consisted of nine APA fellows who served 3-year terms, set and administered standards for professional competence, and awarded diplomas that signified professional recognition of the qualifications of the applicant. At its inception, these standards required the applicant to have: a doctorate in psychology; APA membership; satisfactory moral, ethical, and professional standing; 5 years of professional experience; and passing scores on written and oral evaluations that included samples of the applicant’s diagnostic and therapeutic skills. In 1949, the first ABEPP written examinations were held. (Subsequently, in 1968, this group became the American Board of Professional Psychology, or ABPP).
By 1949, it was generally accepted that the roles of the clinical psychologist were psychotherapy, diagnosis, and research. Since the VA had been involved in so much of the training of clinicians and was a major employer, clinical psychology had gone from being largely a provider of services to children to being largely a provider of services to adults, of whom the majority were males. The membership of the APA had increased to 6,735, and there were 1,047 in the clinical division alone. About 149 graduate departments offered some training in clinical psychology to about 2,800 clinical majors. The profession was growing at a rapid and exhilarating pace.
Subsequent Professional Developments
In 1918, Leta Hollingworth suggested the creation of a new doctoral degree, the PsyD, which could be awarded to psychologists who sought not to be scientists but practitioners of psychology (Hollingworth, 1918). A similar suggestion was made by Crane (1925–1926) with a similar imperceptible response. In 1947, a commission appointed by Harvard University published a report recommending that Harvard establish a PsyD program for clinical psychologists (University Commission to Advise on the Future of Psychology at Harvard, 1947). The report included the following statement, which proved to be somewhat prophetic and a bit comical: “If the best universities deliberately dodge the responsibility for training applied psychologists, the training will be attempted in proprietary schools but under conditions so deplorable that the universities will either be begged to assume responsibility or blamed for not doing so” (p. 33). However, by the time this report was published, the Harvard psychology department had already acted by spinning off a new Department of Social Relations, which included the psychology clinic and its staff and which continued to offer the PhD.
The first institution to offer a PsyD degree was the University of Illinois (Peterson, 1992). It began its PsyD program in 1968 as an alternative for clinical graduate students who might find it more appealing than its PhD program. The PsyD program had a greater focus on training for practice and did not require experimental research; instead, the student could present a detailed case history or a documented attempt at clinical intervention and be prepared to discuss its theoretical, practical, and research implications. Eventually this program was dropped at Illinois and its leading proponent, Donald Peterson, went to Rutgers University to become dean of its Graduate School of Applied and Professional Psychology. (One of the illustrious PsyD graduates of the Rutgers program was Dorothy W. Cantor, president of the APA in 1996.)
In the meantime, the California School of Professional Psychology opened its doors in 1969, offering a 6-year PhD program. Other universities, such as Baylor and Yeshiva, began to offer PsyD programs, and a number of proprietary schools of professional psychology were established, most of which offered the PsyD.
What seemed to spur the growth of PsyD programs was the Vail Conference held in Colorado in 1973 (Korman, 1974). That conference endorsed the practitioner-training model as an alternative to the scientist-practitioner one. But of course there was more to it than that. After the first burst of postwar growth had waned, some universities (e.g., Chicago and Northwestern) had dropped their clinical programs and almost all colleges had far more applicants than they could accept; this alarmed some clinicians into thinking their profession would not be viable until there were independent schools for the training of clinical psychologists. The alarm proved unjustified, as the number of graduate training programs in clinical psychology at universities has continued to increase.As of June 2001, some 50 years after APA approval began, 202 programs were approved or regularly monitored for approval. (Courtesy of Tia Scales at the Education Directorate of the American PsychologicalAssociation.) In addition, 53 free-standing schools wereproducingclinicians(twowerecounselingprograms).In August 1976, these schools banded together into an organization of their own, the National Council of Schools of Professional Psychology, in order to ensure that their interests were pursued and protected (Stricker & Cummings, 1992).
The trend toward state certification and licensure of psychologists reached something like a conclusion when Missouri in 1977 became the last state to enact licensing legislation—though concerns remained about the revocation of laws and legal challenges to them. Clinicians themselves used legal suits to gain admission privileges in hospitals and to be counted as part of medical staffs. Their goals were to compel medical insurance companies to reimburse them for their services and (in 1988 in Welch et al. v. American Psychoanalytic Association et al.) to force an end to the restrictions imposed on lay analysts and their training and practice. Often the APA was involved in this litigation, attesting to a growing involvement in professional issues both within that organization and among clinical psychologists.
In the days of NIMH training grants to PhD programs in clinical psychology, it was considered a policy failure for graduates to enter into independent private practice. Indeed, most of those PhDs took public-sector jobs, whether in teaching, at the VA, or in community mental health centers. That is no longer the case. More and more clinical psychologists are in private practice, and they have promoted the passage of freedom-of-choice legislation, mandating that if insurance companies pay psychiatrists for psychotherapy, they must do the same for clinical psychologists. In a world of managed care, clinical psychologists find themselves competing vigorously for their share of the market. To aid third-party payers in determining which psychologists merit reimbursement, a National Register of Health Service Providers was developed by Carl Zimet and others. To be listed in the register, a psychologist must hold a state license or certification, have successfully completed at least 1 year of internship, and must have 2 years of supervised experience in a health setting.
During the 1970s, the APA was forced to become definitive about what constituted a psychological training program. This came about when graduates of guidance or counseling or sundry other programs demanded to be certified or licensed as psychologists and brought suit if their qualifications were questioned. They asserted, unfortunately correctly, that the courses that went into a psychology education were unspecified. Therefore, the APA made it known that as of 1980 all graduate programs in psychology must require courses in the history and systems of psychology; the biological, social, developmental, and learned bases of behavior; and statistics and research design. Moreover, clinical students were also required to have instruction in psychological assessment and intervention, individual differences and psychopathology, practicum training, and a 1-year full-time internship.
So, what does all this suggest, aside from more regulation and specification than anyone would have thought possible or desirable a few years before? First, clinical psychologists were increasing their numbers and becoming a dominant force within American psychology and perhaps elsewhere as well. They were evident in Canada, the United Kingdom, and Scandinavia. Norway, for instance, was training about 100 psychologists a year at the doctoral level. These countries, unlike the United States, had publicly supported health systems, which were major employers of clinical psychologists.
Although the United States has continued to emphasize a rather lengthy, and somewhat indefinite, period of graduate education leading to the doctorate for clinical psychologists, a variety of other models exist elsewhere. In the United Kingdom, a 3-year program leading to a doctor of clinical psychology degree (D.Clin.Psy.) has emerged. In Germany, Hungary, Mexico, and Spain, the PhD is usually reserved for academicians and/or researchers; practitioners of clinical psychology study in undergraduate-graduate programs lasting up to 6 years, perhaps supplemented by postgraduate training in psychoanalysis or behavior therapy (Donn, Routh, & Lunt, 2000). Believing that it was about time that the largest psychological field of specialization had its own international organization, Routh (1998) and colleagues founded the International Society of Clinical Psychology in 1998. This organization holds its meetings with various larger international groups, such as the International Association of Applied Psychology, the International Council of Psychologists, the International Union of Psychological Science, or the European Federation of Professional PsychologyAssociations.
Second, with increasing numbers come divisions and splits. When there are few psychologists, the interests of one or two can be regarded as idiosyncrasies. When there are thousands of psychologists, the interests of 1% or 2% may constitute the beginning of a new field of specialization or a new social grouping. APA membership has increased from about 7,250 in 1950 to 16,644 in 1959 to 30,830 in 1970 to 50,933 in 1980 to about 150,000 in 2000. At one time, a school psychologist was a clinical psychologist who worked in a school setting, but eventually school psychology became a field of specialization in its own right (Fagan, 1996). Similarly there are more and more areas of specialization within clinical psychology that could become separate fields, such as clinical neuropsychology, clinical child psychology, and health psychology. This differentiation is probably inevitable, but it is not without the possible consequence of fostering less unity among clinicians unless care is taken to ensure cohesiveness.
Third, there has been an increasing professionalization within clinical psychology. Until World War II, very few clinical psychologists were involved in private practice. The role of the clinician changed from one of diagnosis and research to diagnosis, treatment, and research. Correspondingly, along the way from its inception in 1892, the APA’s aim—“to advance psychology as a science”—has changed: “to advance psychology as a science and as a means of promoting human welfare” and “to advance psychology as a science, as a profession, and as a means of promoting human welfare.” As this is being written, the APA membership is being polled on whether “health” should be inserted into the aim of the association. Since many psychologists who objected to the growing professional interests of the APA left it in 1989 to form a more exclusively scientific American Psychological Society and since clinical psychologists constitute more than half the APA membership, the professionalization of the APA is not likely to be reversed. A concern here is that clinicians not become divorced from their scientific roots and function.
Treatment interventions can serve to illustrate much of what we have discussed, and it is to that topic that we turn.
Treatment Interventions
By World War II, many of those who had broken with Freud (such as, Adler, Jung, and Rank) established personality theories, schools, and therapeutic systems of their own that were unified by the importance they ascribed to unconscious motivation in determining psychopathology. These “psychodynamic” psychotherapies were augmented by those of Horney, Sullivan, and Fromm, who, impressed by social forces and relationships, did much to make psychotherapy responsive to changing conditions. Among those just mentioned, Rank and Fromm were not physicians, and both had been trained in Europe. As time went on, Erik Erikson’s (1950, 1959) integration of a psychosocial theory of development with Freud’s psychosexual theory opened psychoanalysis to the concepts of many of the rebels: an oral stage of trust versus mistrust; an anal stage of autonomy versus shame and doubt; a phallic stage of initiative versus guilt; a latency stage of industry versus inferiority; an adolescent stage of identity versus identity diffusion; a young-adult stage of intimacy versus isolation; a middle-adult stage of generativity versus stagnation; and an old-age stage of integrity versus despair.
The first American psychologist to develop a form of psychotherapy that was highly influential was Carl Rogers (1902–1987), who received his PhD in 1931 from Teachers College, Columbia University, where Leta Hollingworth supervised his clinical experiences with children. He continued clinical work with children until 1940, when he left to become a professor of psychology at Ohio State University and later the University of Chicago. By then his clinical work was mostly with college students. Rogers was heavily influenced by social worker Jesse Taft and especially by child psychiatrist and former school psychologist Frederick Allen, who in turn were much affected by what they had learned from Otto Rank. Originally, Rogers called his system of psychotherapy “nondirective” (Rogers, 1942). Later he called it “clientcentered therapy” (Rogers, 1951), and eventually he and his followers referred to it as “person-centered.” No matter what it was called, it was distinguished by Rogers’s willingness to subject it and its practitioners to scientific scrutiny.
Rogers pioneered the recording of therapy sessions so that they could be analyzed in detail for purposes of research, supervision, and training. He argued that psychotherapy could become a science and believed there was a discoverable orderliness as the sessions continued to a successful end. Hypothesis testing was one of the hallmarks of his approach, and he tried to make explicit what conditions were essential for personality change: the therapist’s possession and manifestations of unconditional positive regard, accurate empathy, genuineness, and congruence (Rogers, 1957). A considerable research effort was undertaken to measure these attributes and determine if they indeed were related to effective therapy. The results of 20 years of research led to the conclusion that the relationship between these attributes and positive change in patients remained in doubt (Parloff, Waskow, & Wolfe, 1978).
This period, extending from the 1930s through the 1950s, was the high-water mark in the prestige of psychotherapy, especially psychodynamic psychotherapy. In the 1960s, psychotherapy came under attack from four “revolutions” or “movements”: (1) community psychology, which argued that psychotherapy was futile and not provided to those most in need of it, and that clinicians should direct their efforts toward preventing psychopathology through bringing about changes in deleterious social policies and conditions; (2) humanistic psychology, which emphasized the importance of present experiences, ongoing events, and confrontational approaches in groups, as contrasted with traditionalapproachestotheindividual’sexplorationandintegration of the past; (3) the increasing use of drugs, by physicians and by free spirits, to alter moods, regulate behaviors, and enhance self-esteem and experiences; and (4) behavior therapy.
It was the English clinician Hans Eysenck who was less than enthusiastic about clinical psychologists becoming psychotherapists and raised the question of whether scientific studies had demonstrated the effectiveness of psychotherapy (Eysenck, 1952). Culling the research and pulling together a motley group of studies, he concluded that they failed to demonstrate that control groups were significantly less likely to improve than groups that received psychotherapy. Although psychotherapists strongly disagreed with his conclusion and manner of arriving at it, the fact remained that it was their responsibility to prove otherwise.
In South Africa, psychiatrist Joseph Wolpe made use of Hullian concepts and learning principles to develop procedures that would reduce neurotic symptoms. In essence, he sought to elicit responses, such as relaxation, that would be incompatible with or inhibit a symptom, such as anxiety or fear. (This is similar to the previously discussed deconditioning or reconditioning approach of Mary Cover Jones.) After coming to the United States to spend a year at Stanford University’s Center for Advanced Study in the Behavioral Sciences, Wolpe (1958) published a book, Psychotherapy by Reciprocal Inhibition, which was hailed by Eysenck as a promising advance in effective treatment.
Wolpe took a position at the University of Virginia Medical School, and in 1962, along with Salter and Reyna, sponsored a conference there that got the behavior therapy ball rolling (Wolpe, Salter, & Reyna, 1964). The clinical journals were soon filled with a variety of studies, many of them quite ingenious, demonstrating the effectiveness of behavioral approaches.
One of the first of these studies was one by Peter Lang and David Lazovik (1963) of college students who were identified by a questionnaire, the Fear Survey Schedule, as being afraid of snakes. The students were then given a Behavioral Avoidance Test (BAT) in which they were placed in a room with a nonpoisonous snake and encouraged to go as close as they could to it and, if they were willing, to pick it up. Each student completed a Fear Thermometer, a rating of how much fear was experienced. The therapy consisted of devising a hierarchy of imagined scenes involving snakes, with scenes arranged from neutral to the most fear arousing. Then the student was taught to relax, asked to imagine the least feararousing scene, asked to relax, and so on until the student became able to imagine scenes higher and higher in the hierarchy without feeling anxious, a procedure known as “systematic desensitization.” Finally the BAT and Fear Thermometer were readministered, and it was found that these students had become significantly less afraid of snakes than randomly assigned students in a control group. Critics of such analogue studies noted that the results might have been less impressive had neurotic patients and their fears been tested.
Nevertheless, later research supported the effectiveness of desensitization procedures of various kinds in dealing with a variety of symptoms. For example, exposure with response prevention (allowing a patient to experience what happens when a compulsion is not permitted) is a kind of in vivo desensitization that has come to be regarded as appropriate in the treatment of obsessive-compulsive disorders (Foa & Goldstein, 1978).
Another major behavioral approach to treatment is behavior modification, or applied behavior analysis, which comes from the experimental work and writing of B. F. Skinner (1938).AlthoughSkinner’sexperimentalworkwasalmostexclusively with animals, neither he nor his followers have been reluctant to apply his principles to humans, including clinical populations (Skinner, 1971). Sidney Bijou, who served as director of clinical training when Skinner chaired the psychology department at Indiana University, pioneered in the use of operant conditioning with persons with mental retardation (Bijou, 1996).Applied behavior analysis has become a mainstay of psychological treatment of persons with mental retardation and pervasive developmental disorders such as autism. It has been used to teach social and self-help skills like dressing, toileting, and proper table manners, as well as dealing with defiant, aggressive, and self-injurious behaviors.
Nathan Azrin at Anna State Hospital in Illinois demonstrated the utility of behavior modification with adult mental patients (Ayllon & Azrin, 1968) and the usefulness of token economies, in which the performance of desired behaviors earns tokens that can be exchanged for rewards (much as occurs in our society where money is given for work). Extensive research on token economies in mental hospitals was done by Gordon Paul and his colleagues (e.g., Paul & Lentz, 1977). Their research with long-term, regressed, and chronic schizophrenics focused on developing such practical behaviors as making their beds, behaving well at mealtime, participating in the classroom, and socializing with others during free time. Paul’s research showed that his program of behavior therapy and milieu therapy (moral treatment) improved symptoms when compared with the results of routine hospital management, and that behavior therapy was more effective than milieu therapy alone in bringing about the desired changes.
The principal assessment procedure advocated by Skinnerians is the functional analysis of behavior: a determination of what may be rewarding or maintaining undesirable behaviors and what may serve to reward or establish the performance of behaviors that are desired. A functional analysis requires observation, preferably in the setting where the behaviors are to be modified, in order to assess the frequency of their occurrence and their consequences. Gerald Patterson (1974) pioneered in the use of direct behavioral observations in natural settings to record the behavior of aggressive children and their families in their homes. His research led to a theory of coercion in which the child is seen as both the determiner and victim of episodes of escalating violence in the family and to controlled research on the behavioral treatment of child aggression.
Another major category of behavior therapy is cognitive therapy or cognitive behavior therapy. Two pioneers in this area were George A. Kelly and Albert Ellis. Kelly (1955) viewed his clients as resembling scientists in their attempts to make sense of the world around them. He used a diagnostic procedure called the Role Construct Repertory Test to ascertain their beliefs about themselves and others. The therapist then negotiated with the client about what changes might be desired and how these could be accomplished. Using fixed role therapy, the client was encouraged to rehearse or playact the new role, first with the therapist, then with others. Albert Ellis (1958) developed rational emotive therapy; here the patient’s opinions and attitudes are explored for irrational beliefs (“I can’t make a mistake and must be perfect. My feelings are out of my control”), which the therapist then attempts to make more reasonable and rational.
Martin Seligman (1975) stimulated much research on the treatment of depression. Based upon previous research with dogs that were prevented from avoiding or escaping an electric shock, he noted that when they were in a situation where the shock could not be avoided, such animals simply gave up and endured the pain. They had learned to be helpless, and perhaps, he reasoned, the same process of ineffectiveness and feeling unable to cope occurred among humans who were depressed. This had obvious treatment implications, but further study indicated the need for the concept of attribution (Abramson, Seligman, & Teasdale, 1978): Persons who are likely to become depressed attribute their failures to their own personality characteristics, while those who are not at risk for depression attribute failures to external, transitory, specific circumstances. Accordingly, the cognitive therapist might help a person to be less depressed by coming to see how failures occur in certain situations and dealing with those events more effectively.
Cognitive behavior therapy for treating panic disorders involves teaching the patient to interpret symptoms of acute anxiety as relatively harmless rather than as indications of a pending heart attack or psychotic episode (Craske, Brown, & Barlow, 1991). This was found to be more beneficial than treatment with the anti-anxiety drug Xanax (alprazolam). More recently, Marsha Linehan (1993) developed a procedure, called dialectical behavior therapy, that shows promise in the treatment of borderline personality disorder.
Social learning is yet another major approach in behavior therapy, which owes much to the work of Albert Bandura (1977). The emphasis here is on learning that occurs without obvious rewards, as when we learn what to do by observing the consequences of behaviors performed by others (vicarious learning); or when we imitate the behaviors of those we like, respect, or admire (modeling); or when we have internalized values and standards and reward or punish ourselves for our successes or failures in living up to them, a self-regulating process.
Susan Mineka and her colleagues (Mineka, Davidson, Cook, & Keir, 1984) demonstrated the acquisition of fears in rhesus monkeys through vicarious or observational learning. When adolescent monkeys were allowed to watch their parents, who had an intense fear of snakes, interact with toy snakes and real ones, they soon exhibited the same fear, even though they did not do so originally. Even at a 3-month follow-up, the fear was strongly evident. Similarly, much research was devoted to the consequences of watching violence in movies and television, particularly for producing antisocial, aggressive behaviors in children, which are apt to lead to such behaviors in adulthood (Huesmann, Eron, Lefkowitz, & Walder, 1984). A final example, Peter Lewinsohn’s research (Lewinsohn, 1975, 1988; Teri & Lewinsohn, 1986), demonstrated a correlation between depression and a reduced number of rewards: Losses of any and every kind are risk factors for depression and frequently involve losses of rewards, and a depressed person is less affected by and is less apt to engage in behaviors that elicit social rewards. By helping the person to perform behaviors that generate social rewards, the depression can be alleviated.
Behavioral approaches in treatment have obviously increased rapidly in number and applications. It was not until 1955 that the first course in behavior modification was offered by Arthur Staats, and by the early 1970s about twothirds of the psychology departments in the United States offered behavior therapy courses. It would be rare today for instruction in this topic to be neglected. Equally significant has been its acceptance in medical, psychiatric, and psychodynamic settings. This acceptance has come about because for almost any purpose—reducing stress (Lazarus, 1966), overcoming shyness, modeling appropriate behaviors in the hospital, or applying for a job—training procedures can be helpful. In some circumstances, such as teaching people with retardation or autism, behavioral techniques are among the few means available to provide assistance.
Considerable interest was generated in the study of Smith and Glass (1977), who through a relatively new statistical procedure, meta-analysis, sought to determine if psychotherapy was effective. By reexamining the data from 375 controlled studies of psychotherapy and counseling, they found that typical patients receiving therapy were rated higher than 75% of those in the control groups. They concluded this was evidence for the effectiveness of psychotherapy, though they did not find any support for the superiority of one type of psychotherapy over another.
An alternative or supplement to psychotherapy and behavior therapy is drug treatment.The first neuroleptic medications for the treatment of psychosis were introduced in France in 1952, and by the 1960s they had revolutionized psychiatric treatment.Psychiatry went from shock therapies and custodial care to a “revolving door” policy in mental hospitals that sent patients into halfway houses, where they could be maintained on drugs.This drug revolution—this change in emphasis from “warehousing” patients to avoiding the effects of institutionalization, from isolating them to returning them to society— stimulated the field of community psychology, which was also invigorated by the Community Mental Health Centers Act of 1963. The drugs, particularly chlorpromazine (Thorazine) and other phenothiazines, became widely used all over the world and led to great reductions in the numbers of patientsrequiring hospitalization. Such medications did not necessarily eliminate the psychosis, but they did reduce the severity of symptoms and so helped patients to be more acceptable to others. Some clinicians have been involved in the study of the longterm effects of taking neuroleptics, for example, tardive dyskinesia, a neurological syndrome that involves involuntary movements of the lips and tongue (Sprague, Kalachnik, & Shaw, 1989). Other clinical psychologists have conducted research on the use of both traditional neuroleptics and the newer drugs of this type, for example, risperidone, in the treatment of self-injurious behaviors and aggression in individuals with mental retardation (Schroeder, Rojahn, & Reese, 1997).
A second category of frequently used medications is antidepressants, including tricyclics (Tofranil) and selective serotonin reuptake inhibitors (Prozac). These medications have proven to be effective in many double-blind studies, though not more so than cognitive behavior therapy or manualized interpersonal psychotherapy, according to NIMH clinical trials. Nevertheless, they have brought about a fundamental change in the practice of outpatient psychiatry, which is much more involved with adjusting drug regimens and less involved with psychotherapy than it used to be (Shorter, 1997). Lithium seems an effective treatment for manic states and also has prophylactic value in managing bipolar disorder. Again, while clinicians have made contributions to this area (Jamison, 1992; Jamison & Akiskal, 1983), its administration was a medical responsibility. The same thing can be said about methylphenidate or Ritalin, the most frequently prescribed drug for children, used in the treatment of attention deficit hyperactivity disorder (ADHD). Clinical psychologists have been involved in evaluating the effects of stimulant drugs (Conners, Sitarenios, Parker, & Epstein, 1998) and in determining whether behavior therapy can be an effective treatment. Barkley (1990) used Ritalin to examine the parent–child relations in children with ADHD. The parents of these children tend to be overcontrolling but are less so when their child is on Ritalin, thus indicating they are responsive to their child’s level of hyperactivity. However, not all clinical psychologists were content with restricting their role to research with drugs.
During the 1980s, a movement began to permit clinical psychologists with proper additional training to prescribe these medications. The government sponsored a demonstration project to show its feasibility, and with that accomplished a few university training programs began to offer courses that would prepare clinical psychologists to assume that role. Although the majority of clinical psychologists showed little interest in gaining prescription privileges (Piotrowski & Lubin, 1989), that interest may be more broadly kindled in the coming generations. An APA division for psychologists who do have an interest in prescribing psychotropic medications has been recently established. In 1995 APA Division 12, the Society of Clinical Psychology, set up a task force to identify empirically supported psychological interventions for various types of psychopathology. Such an identification has decided implications for health service insurers, who can use it to determine if practitioners are entitled to be reimbursed for their services. A listing of such treatments tends to endorse behavior therapy approaches more so than psychotherapy, which has led to understandable anguish among psychotherapists, who believe their effects are not fairly evaluated when overt symptoms are the major focus.
The criteria used for selecting empirically supported treatments has been much discussed (Chambless & Hollon, 1998), and an interdiciplinary movement is under way, including representatives of psychiatry, psychology, other mental health fields, managed care executives, and consumers, to develop treatment guidelines so that health care dollars can be rationally allocated.
Conclusions and Future Trends
It should be apparent that clinical psychology has come a long way since 1896. Its growth was slow during the early years of its development when it essentially focused on psychometrics, research, and pedagogical services to children. We should at least mention that the major contribution of clinical psychologists at that time was in the measurement of intelligence. The age scale of BinetSimon led to the revisions of Lewis Terman (the StanfordBinet), longitudinal studies of gifted children (Terman, 1925) that are still being pursued, infant and adult scales that have contributed to our understanding of intellectual functioning throughout the life span, and fairly reliable and valid predictors of success in school, work, and psychotherapy.
Following World War II, clinical psychology grew rapidly until it became a dominant force in American psychology and an established and legally recognized profession with a respected place among the mental health disciplines. Its major contribution in the postwar period has been in treatment formulations, especially behavior therapy approaches.
Clinical psychology is now perhaps the most popular field of psychological specialization in the world (Sexton & Hogan, 1992). With increasing numbers of clinicians has come a trend toward more and more areas of specialization (e.g., school psychology, health psychology, clinical child psychology, pediatric psychology, clinical geropsychology, clinical neuropsychology, family psychology, psychological hypnosis, rehabilitation psychology), many of which have developed into fields of their own (Fagan, 1996; Wallston, 1997). In addition, the practices within the field have expanded, with more sophisticated evaluation techniques, various therapeutic approaches (including use of the electronic medias), and the possibility of prescribing psychotropic medications.
Such growth in numbers and differentiation is to be expected. Nevertheless, care should be exercised to ensure that psychologists are aware of their commonalties—their origins from a common history and their beliefs in a common set of values.
Bibliography:
Abramson, L. Y., Seligman, M. E. P., & Teasdale, J. D. (1978). Learned helplessness in humans: Critique and reformulation. Journal of Abnormal Psychology, 87, 49–74.
Alexander, F. G., & Selesnik, S. T. (1966). History of psychiatry. New York: Harper & Row.
Ayllon, T., & Azrin, N. H. (1968). The token economy. New York: Appleton-Century-Crofts.
Bandura, A. (1977). Social learning theory. Englewood Cliffs, NJ: Prentice-Hall.
Barkley, R. A. (1990). Attention-deficit hyperactivity disorder: A handbook for diagnosis and treatment. New York: Guilford Press.
Beers, C. (1908). A mind that found itself, an autobiography. New York: Longman, Green.
Benjamin, L. T., Jr., & Baker, D. B. (2000). Boulder at 50: Introduction to the section. American Psychologist, 55, 233–236.
Bijou, S. W. (1996). Reflections on some early events related to behavior analysis of child development. Behavior Analyst, 19, 49–60.
Binet, A., & Simon, T. (1905). A new method for the diagnosis of intellectual level of abnormal persons. Annee Psychologique, 11, 191–244.
Breuer, J., & Freud, S. (1955). Studies on hysteria. In J. Strachey (Ed.), The standard edition of the complete psychological works of Sigmund Freud (Vol. 2, pp. 1–305). London: Hogarth Press. (Original work published 1895)
Cattell, J. M. (1890). Mental tests and measurements. Mind, 15, 373–381.
Chambless, D. L., & Hollon, S. D. (1998). Defining empirically supported therapies. Journal of Consulting and Clinical Psychology, 66, 7–18.
Conners, C. K., Sitarenios, G., Parker, J. D. A., & Epstein, J. N. (1998). The revised Conners’ Parent Rating Scale–Revised (CPRS-R): Factor structure, reliability, and criterion validity. Journal of Abnormal Child Psychology, 26, 257–268.
Crane, L. (1925–1926). A plea for the training of psychologists. Journal of Abnormal and Social Psychology, 20, 228–233.
Craske, M. G., Brown, A. T., & Barlow, D. H. (1991). Behavioral treatment of panic disorder: A two-year follow-up. Behavior Therapy, 22, 289–304.
Doll, E. A. (1920). The degree of Ph.D. and clinical psychology. Journal of Applied Psychology, 4, 88–90.
Donn, J. E., Routh, D. K., & Lunt, I. (2000). From Leipzig to Luxembourg (via Boulder and Vail): A history of clinical psychology training in Europe and the United States. Professional Psychology: Research and Practice, 31, 423–428.
Ellis, A. (1958). Rational psychotherapy. Journal of General Psychology, 59, 35–49.
Erikson, E. H. (1950). Childhood and society. New York: Norton.
Erikson, E. H. (1959). Identity and the life cycle. Psychological Issues, 6(1), entire issue.
Eysenck, H. J. (1949). Training in clinical psychology: An English point of view. American Psychologist, 4, 173–176.
Eysenck, H. J. (1952). The effects of psychotherapy: An evaluation. Journal of Consulting Psychology, 16, 319–324.
Fagan, T. K. (1996). A history of division 16 (school psychology): Running twice as fast. In D. Dewsbury (Ed.), Unification through division: Histories of the divisions of the American Psychological Association (Vol. 1, pp. 101–135). Washington, DC: American Psychological Association.
Foa, E. B., & Goldstein, A. J. (1978). Continuous exposure and complete response prevention in the treatment of obsessivecompulsive neurosis. Behavior Therapy, 9, 821–829.
Freud, S. (1926). The question of lay analysis. In J. Strachey (Ed.), The standard edition of the complete psychological works of Sigmund Freud (Vol. 20, pp. 77–172). London: Hogarth Press.
Freud, S. (1959). Analysis of a phobia in a five-year-old boy. In J. Strachey (Ed.), The standard edition of the complete psychological works of Sigmund Freud (Vol. 10, pp. 1–147). London: Hogarth Press. (Original work published 1909)
Gay, P. (1988). Freud: A life for our time. New York: Norton.
Goetz, C. G., Bonduelle, M., & Gelfand, T. (1995). Charcot: Constructing neurology. New York: Oxford University Press.
Hale, N. G., Jr. (1971). Freud and the Americans. Vol. 1: The beginnings of psychoanalysis in the United States 1876–1917. New York: Oxford University Press.
Hilgard, E. R. (1987). Psychology in America. New York: Harcourt, Brace, Jovanovich.
Hollingworth, L. S. (1918). Tentative suggestions for the certification of practicing psychologists. Journal of Applied Psychology, 2, 280–284.
Horney, K. (1937). The neurotic personality of our time. New York: Norton.
Huesmann, L. R., Eron, L. D., Lefkowitz, M. M., & Walder, L. O. (1984). Stability of aggression over time and generations. Developmental Psychology, 20, 1120–1134.
James, W. (1890). Principles of psychology. New York: Holt.
Jamison, K. R. (1992). Touched with fire: Manic depressive illness and the artistic temperament. New York: Basic Books.
Jamison, K. R., & Akiskal, H. S. (1983). Medication compliance in patients with bipolar disorder. Psychiatric Clinics of North America, 6, 175–192.
Jones, M. C. (1924). The elimination of children’s fears. Journal of Experimental Psychology, 7, 382–390.
Kelly, G. A. (1955). The psychology of personal constructs. New York: Norton.
Korman, M. (1974). National conference on levels and patterns of professional training in psychology: The major themes. American Psychologist, 29, 441–449.
Lang, P., & Lazovik, A. D. (1963). Experimental desensitization of a phobia. Journal of Abnormal and Social Psychology, 66, 519–525.
Lazarus, R. S. (1966). Psychological stress and the coping process. New York: McGraw-Hill.
Levine, M. (1981). The history and politics of community mental health. New York: Oxford University Press.
Lewinsohn, P. M. (1975). Engagement in pleasant activities and depression level. Journal of Abnormal Psychology, 84, 644– 654.
Lewinsohn, P. M. (1988). A prospective study of risk factors for unipolar depression. Journal of Abnormal Psychology, 97, 251–284.
Linehan, M. M. (1993). Cognitive-behavior therapy of borderline personality disorder. New York: Guilford Press.
McReynolds, P. (1997). Lightner Witmer: His life and times. Washington, DC: American Psychological Association.
Meltzer, H. (1966). Psychology of the scientist: XVII. Research has a place in private practice. Psychological Reports, 19, 463–472.
Menninger, W. C. (1950). The relationship of clinical psychology and psychiatry. American Psychologist, 5, 3–15.
Mineka, S., Davidson, M., Cook, M., & Keir, R. (1984). Observational conditioning of snake fear in rhesus monkeys. Journal of Abnormal Psychology, 93, 355–372.
Mitchell, D. (1919). The clinical psychologist. Journal of Abnormal Psychology, 14, 325–332.
Mitchell, D. (1931). Private practice. In R. A. Brotemarkle (Ed.), Clinical psychology: Studies in honor of Lightner Witmer (pp. 177–190). Philadelphia: University of Pennsylvania Press.
Morrow, W. R. (1946). The development of psychology internship training. Journal of Consulting Psychology, 10, 165–183.
Mowrer, O. H., & Mowrer, W. M. (1938). Enuresis: Amethod for its study and treatment. American Journal of Orthopsychiatry, 8, 436–459.
Munroe, R. (1955). Schools of psychoanalytic thought. New York: Dryden.
Parloff, M. B., Waskow, I. E., & Wolfe, B. (1978). Research on therapist variables in relation to process and outcome. In S. L. Garfield & A. E. Bergin (Eds.), Handbook of psychotherapy and behavior change. New York: Wiley.
Patterson, G. R. (1974). Interventions with boys with conduct problems: Multiple settings, treatments, and criteria. Journal of Consulting and Clinical Psychology, 42, 471–481.
Paul, G. L., & Lentz, R. J. (1977). Psychosocial treatment of chronic mental patients: Milieu versus social learning programs. Cambridge, MA: Harvard University Press.
Peterson, D. R. (1992). The doctor of psychology degree. In D. K. Freedheim (Ed.), History of psychotherapy: A century of change (pp. 829–849). Washington, DC: American Psychological Association.
Piotrowski, C., & Lubin, B. (1989). Prescription privileges: A view from health psychologists. Clinical Psychologist, 42, 83–84.
Prince, M. (1909–1910). The psychological principles and field of psychotherapy. Journal of Abnormal Psychology, 4, 72–98.
Raimy, V. C. (Ed.). (1950). Training in clinical psychology. New York: Prentice Hall.
Reisman, J. M. (1991). A history of clinical psychology (2nd ed.). New York: Hemisphere.
Report of Committee of Clinical Section of APA. (1935). Psychological Clinic, 23, 1–140.
Rogers, C. R. (1942). Counseling and psychotherapy. New York: Houghton.
Rogers, C. R. (1951). Client-centered therapy. Boston: Houghton Mifflin.
Rogers, C. R. (1957). The necessary and sufficient conditions of therapeutic personality change. Journal of Consulting Psychology, 21, 95–103.
Routh, D. K. (1984, May). When was the first psychology clinic in Iowa founded? Iowa Psychologist, 29, 3–7.
Routh, D. K. (1994). Clinical psychology since 1917: Science, practice, and organization. New York: Plenum Press.
Routh, D. K. (1996). Lightner Witmer and the first 100 years of clinical psychology. American Psychologist, 51, 244–247.
Routh, D. K. (1997). A history of division 12 (clinical psychology): Fourscore years. In D. Dewsbury (Ed.), Unification through division: Histories of the divisions of the American Psychological Association (Vol. 2, pp. 55–82). Washington, DC: American Psychological Association.
Routh, D. K. (1998). Hippocrates meets Democritus: A history of psychiatry and clinical psychology. In A. S. Bellack & M. Hersen (Eds.), Comprehensive clinical psychology (Vol. 1, pp. 1–48). New York: Pergamon Press.
Routh, D. K. (2000). Clinical psychology training: Ahistory of ideas and practices prior to 1946. American Psychologist, 55, 236– 241.
Routh, D. K., del Barrio, V., & Carpintero, H. (1996). European roots of the first psychology clinic in North America. European Psychologist, 1, 44–50.
Routh, D. K., & DeRubeis, R. (1998). The science of clinical psychology: Accomplishments and future directions. Washington, DC: American Psychological Association.
Schroeder, S. R., Rojahn, J., & Reese, M. R. (1997). Reliability and validity of instruments for assessing psychotropic medication effects on self-injurious behavior in mental retardation. Journal of Autism and Developmental Disabilities, 27, 89–102.
Seligman, M. E. P. (1975). Helplessness: On depression, development, and death. San Francisco: Freeman.
Sexton, V. S., & Hogan, J. S. (1992). Epilogue. In V. S. Sexton & J. D. Hogan (Eds.), International psychology: Views from around the world (pp. 467–477). Lincoln: University of Nebraska Press.
Shakow, D. (1965). Seventeen years later: Clinical psychology in the light of the 1947 Committee on Training in Clinical Psychology report. American Psychologist, 20, 353–362.
Shakow, D. (1976). Reflections on a do-it-yourself program in clinical psychology. Journal of the History of the Behavioral Sciences, 12, 14–30.
Shorter, E. (1997). A history of psychiatry: From the era of the asylum to the age of Prozac. New York: Wiley.
Skinner, B. F. (1938). The behavior of organisms: An experimental analysis. New York: Appleton-Century-Crofts.
Skinner,B.F.(1971).NewYork:Knopf.
Smith, M. L., & Glass, G. V. (1977). Meta-analysis of psychotherapy outcome studies. American Psychologist, 32, 752–777.
Sprague, R. L., Kalachnik, J. E., & Shaw, K. M. (1989). Psychometric properties of the Dyskinesia Identification System: Condensed User Scale. Mental Retardation, 27, 141–148.
Stricker, G., & Cummings, N. A. (1992). The professional school movement. In D. K. Freedheim (Ed.), History of psychotherapy: A century of change (pp. 801–828). Washington, DC: American Psychological Association.
Teri, L., & Lewinsohn, P. M. (1986). Individual and group treatment of unipolar depression: Comparison of treatment outcome and identification of predictors of successful treatment outcome. Behavior Therapy, 17, 215–228.
Terman, L. M. (1925). Genetic studies of genius. Stanford, CA: Stanford University Press.
University Commission to Advise on the Future of Psychology at Harvard. (1947). The place of psychology in an ideal university. Cambridge, MA: Harvard University Press.
Wallston, K. (1997). A history of division 38 (health psychology): Healthy, wealthy, and Weiss. In D. Dewsbury (Ed.), Unification through division: Histories of the divisions of the American Psychological Association (Vol. 2, pp. 239–267). Washington, DC: American Psychological Association.
Watson, J. B. (1913). Psychology as the behaviorist views it. Psychological Review, 20, 158–179.
Watson, J. B., & Raynor, R. (1920). Conditioned emotional reactions. Journal of Experimental Psychology, 3, 1–14.
Witmer, L. (1897). The organization of practical work in psychology. Psychological Review, 4,
Witmer, L. (1907a). A case of chronic bad spelling: Anesia visualis verbalis, due to arrest of post-natal development. Psychological Clinic, 1, 53–64.
Witmer, L. (1907b). Clinical psychology. Psychological Clinic, 1, 1–9.
Witmer, L. (1909–1910). The restoration of children of the slums. Psychological Clinic, 3, 266–280.
Witmer, L. (1925). Psychological diagnosis and the psychonomic orientation of analytic science. Psychological Clinic, 16, 1–18.
Wolpe, J. (1958). Psychotherapy by reciprocal inhibition. Stanford, CA: Stanford University Press.
Wolpe, J., Salter, A., & Reyna, L. J. (Eds.). (1964). The conditioning therapies: The challenge in psychotherapy. New York: Holt, Rinehart and Winston.
Yerkes, R. M. (1919). Report of the Psychology Committee of the National Research Council. Psychological Review, 26, 83– 149.
Yerkes, R. M., Bridges, J. W., & Hardwick, R. S. (1915). A point scale for measuring mental ability. Baltimore: Warwick & York.