
View sample public health research paper on public-private mix in health care systems. Browse research paper examples for more inspiration. If you need a thorough research paper written according to all the academic standards, you can always turn to our experienced writers for help. This is how your paper can get an A! Feel free to contact our writing service for professional assistance. We offer high-quality assignments for reasonable rates.
General Considerations
The theme of public–private partnerships in public health and health-care systems has become remarkably prominent since the 1970s. More generally, the contrast between the role of public and private organizations in providing health services has become an extremely important part of discourse and debate internationally. Much of this discourse proceeds as if the distinction between public and private organizations, and their respective roles in health care, were clear and distinct. A broad definition of public organization is one with a mandate for delivering public goods. A narrower and more common definition of public requires that the organization be a governmental entity. Yet close inspection reveals a great diversity of definitions of public and private in health care and a great diversity of approaches to public and private partnership in public health. Moreover, the definitions of public and private are constantly evolving and, most interestingly, we see a constant hybridization of the public and private efforts in health care.
Academic Writing, Editing, Proofreading, And Problem Solving Services
Get 10% OFF with 24START discount code
If the definitions of public and private in health care are so fluid, how and why is the literature on the ideal public–private mix so strident? The simplest explanation is that the terms public and private are always defined relative to each other, and that they refer to real opposing social movements in specific contexts. Those opposing movements are rooted in neoliberalism and its resistances, both of which have taken hold all over the world but always in a unique form, reflecting specific local political contexts (Leitner et al., 2007). Therefore, one productive way to understand the meaning of public and private in health care and its underlying dynamics is to contextualize health care within various forms of the neoliberal agenda, which seeks to find market solutions to health-care problems, and the opposing movement of resistance, which seeks to preserve if not expand the public role in health care. While it is most common to advocate for public–private partnerships, some oppose this as a dilution of the unique public role in health. Still others enthusiastically promote privatization as a means of increasing efficiency and lowering cost of health services. The advocates of these opposing perspectives usually assume their audiences understand the meaning between public and private. In some cases, public is taken as synonymous with governmental, and private is reserved for nongovernmental. Others use private to denote for-profit organizations, with nongovernmental not-for-profits falling into a separate category, a third sector, that is not necessarily public or private. Reich (2002) notes that some international nongovernmental organizations, such as Me´dicins Sans Frontie`res and Helen Keller International belong to such a third sector, or civil society. These organizations are private in that they are not part of a governmental structure, but are public in the sense that their purpose is to promote the common good. He concludes that such nongovernmental organizations belong to civil society, a third sector (Reich, 2002: 3–4).
Reich’s flexible approach to defining the public and private recognizes the inherently blurry boundaries between these categories and the pragmatic necessity of considering a third sector. Another example of a flexible and pragmatic approach to defining the public and private was taken in a conference on public–private partnerships for public health in Africa (Hursh-Cesar et al., 1994). The conference concluded not only that a typology of the public and private in public health would necessarily vary from one country to the next, but also that the definitions could reflect the interests of those who have the power to define. Therefore, they believe it is important to ask ‘‘who would define the typology – the public sector or the private providers themselves? Would it clarify ownership and control of services?’’ (Hursh-Cesar et al., 1994: 18–19).
Another approach to understanding public and private efforts in health care is to see these as outgrowths of basic human impulses for individual and collective well-being. Taking this general perspective, the private sector relies more on individual interests in preserving well-being and individual profiting from providing healing services to paying clients. The collective interest in preserving the health of a group is the basis for the development of public health services, meaning those that cannot be consumed individually but rather that benefit the public as a whole. The latter would include not only public goods such as clean water, clean environment, and safe collective food supplies, but also collective pooling of resources to ensure against the catastrophic loss associated with illness. Modeling private and public health in terms of individual and collective interests has the virtue of highlighting the conflicts between those interests. Classic examples of conflicts between individual and collective interests, also known as social dilemmas, include the likelihood that some individuals will free-ride on public generosity, taking advantage of collectively shared goods by not contributing or shirking one’s responsibilities, for example not paying health premiums or taxes, or over utilizing services or a scarce public good such as clean water.
It is reasonable to assume that individual interest in well-being and individual strategies to preserve health probably existed well before our records of healing systems. Yet it is just as reasonable to assume that collective action for health also has a very long history, because the illness of any given individual has ramifications for every other member of the group, most obviously when disease is contagious. Yet different societies have different traditions for sharing public goods and, obviously, very different healing systems have evolved internationally. The modern health sector has roots in more ancient health and healing systems, which were themselves a mixture of both privately and publicly owned entities. Hence, the challenges of integrating the private and public sectors in health care is not a new phenomenon at all. Most contemporary healing systems include both private healers and at least some system for assuring collective health. Different societies have struck a different balance between private and public healing modalities, resulting in different types of complex health systems. Depending on the political ideology that has predominated, the health system developed in different ways in different nations. In certain countries, the state exercised their authority on the provision of health care to the people and developed a predominantly state-controlled service sector. In other countries, in contrast, the state has a minor involvement in managing health systems. In other societies, the political ideology affecting health care has changed, and the evolution of health systems has paralleled those broader ideological shifts.
Public health systems are not restricted to services provided by the governmental services or infrastructure, because private providers are inextricably part of public health systems. Private providers of many different types are in innumerable ways part of public health-care systems. In many countries at least, public health systems include dense networks of private and public providers of many different types that interact in complex ways on a daily basis. For example, when HIV-AIDS surfaced, public and private organizations often developed public–private partnerships to provide new services. HIV services, often carried out by private organizations, had to coordinate with HIV testing and reporting, the latter generally carried out by public providers and authorities.
No system is just an aggregate of the parts and, likewise, public health systems should not be seen as a list of services and functions. Public and private health providers interact in many ways. The great challenge is for the two sectors to find better ways to interact, to together become a viable system so that responses to public health crises, particularly sudden unanticipated ones, can be coordinated. One general model of understanding the ideal public–private mix, is the reinventing government approach popular in the United States, Britain, and several other nations. That model promotes many forms of promoting competition, including putting out competitive bids open to private and public providers, but also including many other ways of promoting competition. However, much of public health-care services may not benefit from such models, because public health involves provision of public goods that cannot be individually consumed, and also involves very high levels of professional expertise that does not thrive in competitive markets. Many public health and health-care organizations have actively been trying to get different stakeholders to share responsibility, not just turn it over to the private sector. The later concept is often referred to as a public–private partnership.
Public–Private Partnerships In Health Care
A public–private partnership (PPP) includes the following fundamental features:
- Includes at least two major partners, one representing a public entity established to deliver public goods and a second partner that is a nongovernmental organization, that intend to collaborate.
- The collaboration should lead to sharing of resources in improving the delivery of an intended public good.
- Both parties should be able to benefit by the collaboration while being accountable for the decisions made and outcomes achieved.
A simple partnership is often defined as the sharing of risks and rewards (included in items two and three above), while a public–private partnership (PPP) also needs to include explicit concern for meeting public needs and public accountability. It is important to note that some (e.g., Reich, 2002) define PPP as necessarily including a for-profit entity, while many others use a less restrictive definition that includes not-for-profits. Many parties in different capacities can be involved in the partnerships provided there is agreement on fundamental principles. Involvement of nongovernmental organizations (NGOs) between the partnerships of governments and private sector is commonly seen. NGOs can serve as facilitators of the partnership or as co-partners in pursuit of the objective of the partnership. The NGO may provide resources or expert guidance, as is the case of the World Health Organization. The best approach for public–private partnerships depends on factors such as:
- political ideology of the country or organization;
- organizational structure of the country or organization;
- primary focus (e.g., national, international);
- primary function – curative or preventive;
- modes of financing;
- possible private sector partners (e.g., are there sufficient private providers in the geographical area?);
- international agreements, e.g., GATS, TRIPS.
The political ideology of the government or the organization plays a major role in deciding the extent to which the private sector will be incorporated. Governments that insist on maintaining major responsibility for health may limit their partnerships to the outsourcing of nonclinical minor functions of the health services. A more liberal political setup would offer private sector to build joint ventures in hospital development and management.
The organizational structure of a country’s public health system will spell out the possible mechanisms of integration of private stakeholders into the existing system for providing health services. For example, in a centrally controlled health system, partnerships need to be built at the center of decision-making if private stakeholders are to have a significant role in decision-making as well as in implementation.
Many consider certain international organizations such as the World Health Organization as more closely resembling public rather than private organizations. International organizations such as the WHO may negotiate partnerships with private partners with an international reach, as well as with private partners limited to one nation. The WHO has the competency and resources necessary to successfully undertake such large-scale partnerships. One of the best examples of the latter are the global partnerships developed with pharmaceutical companies producing vaccines against preventable infectious diseases. International organizations can partner with the pharmaceutical industry to purchase large quantities of vaccines, drugs, or other supplies. The purpose is to provide and distribute these products to underserved populations in less developed countries that cannot afford to buy them at the market prices. This guarantees a reliable market for the industry, through public provision of incentives for private research and development of drugs and vaccines. Such large-scale partnerships may reduce the cost of vaccines to populations in poor countries in a relatively short period of time. The international agency may withdraw its subsidy when the price of such drugs and vaccines has reached a level affordable by the recipient country.
Building public–private partnerships for preventing disease differs in many ways from more profit-oriented partnerships. For-profit private sector involvement in preventive efforts is generally low due to low financial incentive. However, the private sector involvement in preventive health efforts often has proven vital for long-term success. Elimination of vaccine-preventable illness in childhood in many countries was achieved with partnerships with private physicians. These private physicians collaborated with the public health authorities in reporting cases while the state provides free vaccines.
The mode of financing in public health is a key factor that determines the nature of many public–private partnerships. Funding to run public health systems could come from general national revenue, special taxes for developing the health sector, nominal user fees, social security systems, other health insurance systems, or foreign aid. Fiscal policies of the government or the organization will determine the extent of involvement of private investments and private sector participation in public enterprise. Policies for restricting private ownership in public facilities, public oversight of insurance systems, financial management in public health institutions, and payments for outsourcing of certain services in public facilities will all depend on the financing mechanisms.
Approaching the correct private partner is crucial for the success of any partnership. The private sector partner should be able to accommodate the common objective of improving the public good while attaining their own corporate objectives. For example, a private for-profit organization’s incentives should not significantly differ from that of the public organization, or else the private entity may end up compromising the partnership. It is important not only to identify the explicit mission of both organizations, but also the implicit incentives. The private sector often expresses interest in certain subsectors that are more attractive to them financially, such as hospital services. However, it is often difficult to enroll partners for less attractive fields as preventive programs forcing the public sector to be more flexible on selection criteria. Private partners may believe they can turn a profit by restricting provision of needed services, especially if public monitoring is unfeasible or otherwise inadequate.
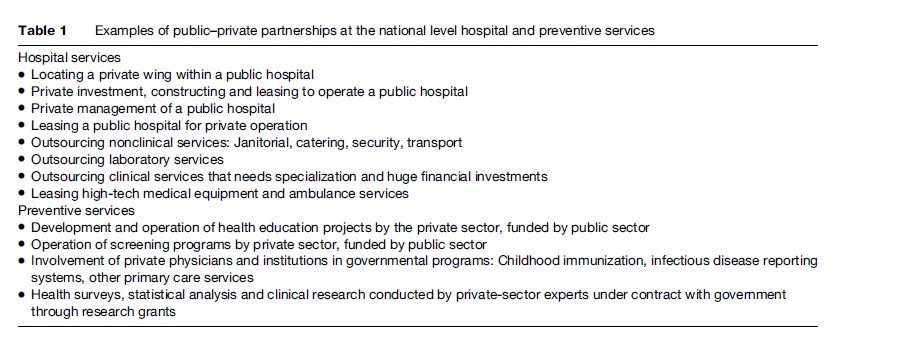
International trade agreements such as General Agreement of Trade in Services (GATS) currently influence public–private partnerships. State-operated services are not considered under the purview of the GATS agreement in that they provide noncompetitive and noncommercial services. The World Trade Organization may view some public–private partnerships as competitive and commercial depending on the nature of the arrangements under the partnership. Hence, the general rules of GATS, Most Favored Nation, National Treatment and Market Access, may apply to services provided by public–private partnerships in the health sector. These clauses are major concerns when deciding the nature of the partnerships in order to improve the health sector while safeguarding the national or organizational interest (Table 1).
Examples Of Public–Private Mixes
The following are few examples of public–private mixes from both developed and less developed countries.
Public–Private Financing And Private Provision Of Services In South Korea
South Korea employs public–private financing of primarily privately provided health care. Although publicly financed private provision is common in many other countries, the Korean case is a rather extreme example of private domination of provision. Over 90% of medical institutions are private, over 90% of total beds are private, and over 90% of specialist physicians are private. Moreover, the private provision is not strictly regulated and patients have great freedom of choice (Jeong, 2005). The free-market approach there may be responsible for disparities between rural and urban regions in access. While 80% of the population lives in rural regions, 90% of the physicians and beds are in urban areas (Jeong, 2005: 135). Yet, on the demand side, the Korean government maintains a great deal of control over fee setting, while financing is funded through a mix of private and public sources (Jeong, 2005). The government public health system in South Korea has employed district health information systems since the early 1990s to help local authorities plan and manage comprehensive health-care services and to help the central government plan services nationally (Dongwoon and Heejin, 2003).
Tuberculosis Control In India
In India, the tuberculosis control program has used public–private partnerships to improve the accessibility and quality of services to the population in case reporting, screening, and providing treatment for diagnosed patients. As reported by Dewan and colleagues (2006), the partnership between the Indian government and private practitioners has increased the case notification rate.
Public–Private Mix In Canada
Private health care in Canada is essentially anything over and above what the public system will reimburse. What the public system will finance is regulated by the Canada Health Act. The Canada Health Act assures that all eligible people in the country have access to insured prepaid health services. This is essentially public health insurance. The Canada Health Act also assures that health-care coverage in the provinces is:
- Portable: Citizens that move from one province or territory to another do not lose coverage.
- Universal: All insured residents of a province or territory must be entitled to the insured health services provided by the provincial or territorial health-care insurance plan.
- Accessible: ‘insured persons in a province or territory have reasonable access to insured hospital, medical and surgical-dental services on uniform terms and conditions.’ (Overview of the Canada Health Act, Accessibility, Section 12: http://www.hc-sc.gc.ca/hcs-sss/mediassur/cha-lcs/overview-apercu_e.html)
However, some provinces in Canada allow doctors to practice outside the public system, although many require that physicians charge the same or less than what the government would pay for the services under the publicly insured system. Many provinces are seeing an increase in health-care providers practicing outside the provincial system. For example, Quebec has seen significant growth in private, for-profit clinics. Some provinces, such as Ontario, have attempted to strengthen the public system.
Canada spent an estimated $142 billion on health care in 2005, according to Health Care in Canada 2006, a report released by the Canadian Institute for Health Information. Of that, just over $98.8 billion was spent by governments delivering public health care. Approximately $43.2 billion was spent on private health care. However, much of the health care is delivered by private providers while funded by the government. Many of Canada’s privately run hospitals and clinics are funded through their provincial government. According to the former president of the Canadian Medical Association, 75% of health-care services are delivered privately, but funded publicly.
Frontline practitioners, whether they’re GPs or specialists by and large are not salaried. They’re small hardware stores. Same thing with labs and radiology clinics … The situation we are seeing now are more services around not being funded publicly but people having to pay for them, or their insurance companies. We have sort of a passive privatization.
Dr. Albert Schumacher, 2006, CBC News Report
Several of the newer clinics now operate on a for-profit basis. Some have argued that a trend would damage the public health-care system. Yet in 2006, the Conservatives government proposed a mix of public and private health care, in which an expanded base of private providers would remain publicly funded and universally accessible. As a result, Canada has recently seen much debate about the pros and cons of shifting toward more private health care. Some argue that more private health would not threaten the public system, but rather will expand the health-care choices for those who can afford to pay for care over and above what is publicly financed. They argue the public system will be maintained and that more choice does not mean one system for the rich and one for those who cannot afford to pay extra.
Public And Private Health Insurance In The United States
The health care of most United States citizens is financed through a mix of public and private programs. The majority of citizens receive health-care benefits through private employers. Employment-based health-care coverage arose largely in the years after World War II, when many employers began to provide health-care benefits to workers in response to Federal Government wage controls.
Public funding for health care rose dramatically in 1965, when Congress established Medicare and Medicaid, through passage of the Social Security Act. The Medicare Program covered most persons aged 65 or older. The Medicaid Program extended federally funded cash assistance programs for the indigent. Medicaid is funded jointly between the Federal and State governments. Each state administers somewhat unique Medicaid policies, although they are constrained by the general guidelines enforced by the Federal Government. Eligibility has expanded over the years (Rowland and Garfield, 2000). Congress established the State Children’s Health Insurance Program (SCHIP) in 1997 to encourage States to extend Medicaid eligibility to a greater number of uninsured children (U.S. Department of Health and Human Services, 2001; Centers for Medicare & Medicaid Services, 2002).
Most of the recent proposed solutions to the problem of rising numbers of the uninsured have focused on making private insurance more affordable, rather than merely extending public coverage. Politicians and policy makers have recently proposed new mixes of public and private programs and policies, including tax credits for low-income uninsured and public funding for persons in very high-risk pools. These proposals generally modify or supplement, rather than replace, the existing private employment-based coverage. Payment for many types of health-care coverage by private employers has decreased. Employer-sponsored retiree coverage has decreased since the mid-1990s. The proportion of health-care costs paid for by private employers is likely to continue to decrease, and public coverage may not be able to cover the difference. As a result, the individual health-care consumer will share more of the burden in the form of increased co-payments and higher insurance premiums. That is, the proportion of private individual payments will increase as private employer-based payments decrease. Increases in premiums have led many individuals to drop health-care coverage entirely, contributing to increases in the numbers of uninsured.
Public policies emerge to fill in some of the gaps to private coverage, but then new private coverage policies emerge as potential solutions to the remaining gaps. For example, many significant gaps in Medicare coverage persist. One of the most important remaining gaps in Medicare is the lack of coverage for long-term care services. Thus most Medicare beneficiaries look to supplemental coverage from various public and private sources. Medicare covered 56% of personal health-care costs for its beneficiaries in 1997. Yet some personal healthcare expenditures are for services not covered by Medicare such as long-term care and dental services. Even when services are paid for in part by the government, beneficiaries often must pay a portion of the costs. This co-payment requirement is also a substantial financial barrier to care for Medicare-covered services. For all these reasons, beneficiaries often are advised to seek out supplemental coverage. Beneficiaries with no supplemental coverage are much more likely to delay care due to cost compared with other beneficiaries (Shatto, 2001). Changes in private and public health insurance, and changes in the relationship between them, are important for policy makers to understand.
Privatization Of Public Health
Conventional wisdom has been that privatization is carried out when available financial resources are decreased. This rests on the assumption that decision makers believe private provision of services is cheaper if not more efficient, and that decision makers believe the cost or efficiency factor is more important than other considerations in deciding whether or not to privatize. Evaluation of the benefits and costs of public health service delivery, however, involves decisions that go far beyond short-term costs and benefits. Many public health services are oriented to prevention of disease or to preparedness for unexpected outbreaks. Such services cannot be evaluated simply in terms of simple measurements of health outcomes and costs. Moreover, although it is often touted as a way of avoiding governmental bureaucracy, the contracting out of public services often produces its own organizational complications (Sclar, 2000). Additional managerial time and resources in the form of paperwork, oversight capacity, and other transaction costs are associated with privatization (Keane et al., 2001). This may explain why Rehfuss (1989) found that any costs savings due to privatization have generally been in single digit percentages. Thus there is preliminary evidence that public health privatization often does not have the conventionally expected effects on costs or efficiency. Nor is there good evidence that privatization is carried out as a response to declining resources. For example, a survey revealed that privatization of public health services in the Unites States resulted in increased time devoted to management and resulted in only modest costs savings, from the perspective of health department directors (Keane et al., 2001).
Privatization Of Public Health Department Services In The United States
Within the field of public health in the United States, there have been efforts to focus local health department (LHDs) on what has been considered the unique mission of public health, what the APHA in 1940 called ‘desirable minimal functions’ (Terris, 1949) and what since 1988 have been called core functions – assessment, assurance, and policy making – which have been further articulated into ten essential public health services. Since the 1970s, there has been an increasing emphasis in the managerial literature on the desirability of more tightly focusing organizations around their core mission. The core functions of public health represent an important managerial framework for defining the unique mission of governmental health departments (Koplin, 1990; Wall, 1998; Keane, 2005). Judging from references to the concept in publications as well as professional practice (Institute of Medicine, 1988; Baker et al., 1994), the core functions have become a central paradigm in the profession of public health. The concept of core functions directly bears on decisions to discontinue provision of services. Many believe that a critical issue confronting public health concerns the extent to which LHDs should withdraw from the direct provision of services, particularly for personal health care, in order to focus on the core functions (Wall, 1998).
Several decades ago, many LHDs in the United States began to increase their provision of personal health services, because they perceived that low-income populations did not have adequate access to such services from other providers (Wall, 1998). While some policy makers and public health officials believe that LHDs should focus exclusively on performance of core functions – assessment, assurance and policy making – and disengage from direct provision of personal health services, the vast majority of today’s LHD directors use a more complex strategy in which they directly provide personal health services in when they believe the uninsured do not have adequate access to such services elsewhere.
Unfortunately, there are reasons to suspect that LHDs’ capacity to provide personal health services has been eroding. Like many health-care providers, LHDs often have not received adequate funds to cover indigent care, despite increases in the numbers of uninsured. Many health-care providers, including LHDs, have become dependent on Medicaid revenues to enable them to provide care to the uninsured. Increases in Medicaid managed care, however, may have diverted Medicaid clients away from LHDs. Medicaid managed care is a privatization of the network formation aspects of Medicaid in that states contract with managed care organizations to provide care to a segment of the Medicaid population. Public health-care organizations such as LHDs are less likely to be included in managed care networks or designated as primary care providers. For these reasons, increases in Medicaid-managed care may have diverted Medicaid clients and revenues away from LHDs, a privatization of LHD Medicaid revenue. Thus, increased enrollment in Medicaid-managed care may be associated with a reduction of the ability of organizations, such as LHDs, to provide health-care services to the uninsured.
Two general types of privatization of health departments are occurring in the United States. One form of privatization occurs when a service once directly performed by an LHD is contracted out to a private provider. Another, less commonly recognized form of privatization occurs when an LHD becomes involved with a new service but contracts out (or otherwise delegates) the performance of the service from its inception.
By the end of the 1990s, more than one-half of health departments (57%) were delegating out the direct performance of at least one service that was formerly performed within the health department (Keane et al., 2001). About one-half (52%) had contracted out at least one public health service from the very inception of the service. Almost three-quarters (73%) of local health departments had privatized some public health service, whether a formerly in-house or not formerly in-house service. Indeed, most health departments have privatized more than one service, often a combination of services formerly performed in-house and services contracted out from their inception. LHDs that had privatized any given category of services were more likely to privatize services from the other service categories (Keane et al., 2001).
A total of 21% of all LHDs had discontinued provision of some personal health service. Discontinuation was defined as termination of all service provision by the LHD with no arrangement made for other providers to take over these services. Of all LHDs, 15% discontinued some HIV services, 5% discontinued some maternal and child health (MCH) services, and 5% discontinued other personal health services. Discontinuation of MCH services was significantly higher among LHDs that lost a large proportion of Medicaid clients to private providers (Keane et al., 2003).
A similar trend of privatization had occurred among public hospitals in the United States. Between 1985 and 1995, the total number of public hospitals declined by 14%. During those years, 165 public hospitals closed, and 293 public hospitals converted to private ownership, and 20 more public hospitals converted to private ownership but closed very soon afterward. This privatization of hospitals raises some of the same concerns associated with the privatization of public health departments. Even more so than health departments, public hospitals are often considered providers of last resort. For those who cannot receive health-care services elsewhere, public hospitals have served as a safety net, meaning that they generally serve the uninsured or underinsured without expectation of payment (Legnini et al., 1999). Therefore, closure and conversion of public hospitals may very well be associated with lower overall access for vulnerable populations, especially as the numbers of uninsured persons increase.
Problems And Difficulties Encountered In Mixing Private And Public
Public and private are historically viewed as two distinct domains despite numerous interconnections in operation. Thus, the main challenge is in getting these sectors together in defining a common agenda. This is particularly challenging given the fact that the basic objectives of each setup, the mandate they have, the organizational structure, the financing mechanisms, the management strategies, the nature of the employees, and the anticipation of outcomes by clients from the two sectors are different in many ways. Since harmonization of those different elements in the process of negotiation for a common agenda is needed in building a fruitful partnership; initial difficulties start from the stage of framing the policies of both sectors. Thus public–private partnerships require an attitude of transformation in policy making.
In framing the PPP, it is vital to define the ground rules of the partnership. Public–private partnership is not handing over the entire public responsibility to the private sector. It is rather a means of increasing the efficiency of the delivery of public goods and improving the sustainability of such services through a mutual arrangement of responsibilities to each party. Public and private sectors have their own strengths and weaknesses. Hence, the rationale is to utilize the optimal capabilities of each partner to produce a synergistic effect in achieving the objectives. Although privatization and public–private partnerships are two different entities, it is a prerequisite to define and frame the independent identities of the two sectors while explicitly presenting the extent of interaction of the sectors in achieving the common goal for the betterment of health of the people. Defining the responsibilities and stakes of both parties at the very beginning will help to minimize most of the problems relating to accountability, trust, and cooperation of public and other interested parties in the stage of actual operation.
In laying the policy framework and operational strategies for the partnership, the presence of a strong public sector is certainly an advantage. At the same time, the private partner needs to be involved in the decision-making process. Participatory decision making enables both parties to counterbalance each other’s interests while harmonizing the power structure between the two. This provides shared responsibility for the decisions made and minimizes accountability issues in the long run. It is vital to assess the ability of the partners to sustain the commitment in the initial stages of negotiation. A regulatory process for public–private partnerships within the broader policies of the state with arbitration procedures needs to be in place. All actions in the partnership should ensure transparency and be accountable to the public. The private sector incentives and stakes in the partnership need to be explicit, as does the extent of control retained by the public sector. Legislative enactment of regulatory procedures and governance structure of the partnership will prevent any shift toward cessation of responsibilities of the public sector toward health. Such operational arrangements should alleviate most of the common problems encountered in public–private partnerships.
Bibliography:
- Dewan PK, Lal SS, Lonnorth K, et al. (2006) Improving tuberculosis control through public-private collaboration in India: Literature review. British Medical Journal 332: 574–578.
- Dongwoon H and Heejin L (2003) District health information systems in the public sector: Health centres in Korea. Logistics Information Management 16: 278–285.
- Goody B, Mentnech R, and Riley G (2002) Changing nature of public and private health insurance. Health Care Financing Review 23(3): 1–7.
- Hursh-Cesar G, Berman P, Hanson K, Rannan-Eliya R, and Rittmann J (1994) Private and Nongovernment Providers: Partners for Public Health in Africa. Conference Report, 1994, Nairobi, Kenya. Institute of Medicine Committee for the Study for the Future of Public
- Health (1988) The Future of Public Health. Washington, DC: National Academy Press.
- Jeong HS (2005) Health care reform and change in public private mix of financing: A Korean case. Health Policy. 74: 133–145.
- Keane C (2005) The effects of managerial beliefs on service privatization and discontinuation in local health departments. Health Care Management Review 30(1): 52–61.
- Keane C, Marx J, and Ricci E (2001) Perceived outcomes of privatization in local health departments. Milbank Quarterly 79(1): 115–137.
- Keane C, Marx J, and Ricci E (2003) Local health departments’ mission to the uninsured in the age of managed care: Results of a national survey. Journal of Public Health Policy 24(2): 130–149.
- Legnini MW, Anthony SE, Wicks EK, Meyer JA, and Rybowski Stepnick LS (1999) Privatization of Public Hospitals. Washington, DC: Henry J Kaiser Family Foundation.
- Rehfuss J (1989) Contracting out in government: A guide to working with outside contractors to supply public services. San Francisco, CA: Jossey-Bass Publishers.
- Reich MR (2002) Public-Private Partnerships for Public Health. Cambridge, MA: Harvard University Press.
- Rowland D and Garfield R (2000) Health-care for the poor: Medicaid at 35. Health Care Financing Review 22(1): 23–34.
- Schumacher A (2006) Health Care: Private Versus Public. CBC News Report August 21, 2006.http://www.cbc.ca/news/ background/healthcare/public_vs_private.html (accessed November 2007).
- Sclar ED (2000) You don’t always get what you pay for. The economics of privatization. Ithaca, NY: Cornell University Press.
- Shatto A (2001) The Characteristics and Perceptions of the Medicare Population. Data from the 1999 Medicare Current Benificiary Survey. Baltimore, MD: Health Care Financing Administration.
- Terris M and Kramer N (1949) Medical care activities of full-time health departments. American Journal of Public Health 39: 1125–1129.
- S. Department of Health and Human Services (2001) 2001 HCFA Statistics HCFA Pub. No. 0(3427).
- Wall S (1998) Transformations in public health systems. Health Affairs 17: 65–89.
More Public Health Research Paper Examples:
ORDER HIGH QUALITY CUSTOM PAPER

Always on-time

Plagiarism-Free

100% Confidentiality