
View sample successful aging research paper. Browse research paper examples for more inspiration. If you need a psychology research paper written according to all the academic standards, you can always turn to our experienced writers for help. This is how your paper can get an A! Feel free to contact our writing service for professional assistance. We offer high-quality assignments for reasonable rates.
What is successful aging? At first glance, this seems like an easy enough question. After all, don’t all humans want to be happy, healthy, wealthy, and beloved well into old age? However, considering that older people are very likely to face health-related problems, maybe healthy should be skipped from the list. Similarly, when people advance into very old age, the loss of their spouse or partner and of close friends is the norm rather than the exception. Considering this, beloved might take on a meaning in old age that is different from that in younger age groups. Finally, happiness seems such an elusive state that we might not want to make this the criterion for successful aging. Maybe it is not so easy to answer the question of what successful aging is after all.
Academic Writing, Editing, Proofreading, And Problem Solving Services
Get 10% OFF with 24START discount code
In this research paper, we approach the concept of successful aging from three different perspectives:
- We first focus on the context of old age. What are the external and internal changes that distinguish old age from younger age groups? What are the characteristics that might render old age a time in life that is feared rather than hoped for? Why is it (as the saying goes) that everybody wants to get old but nobody wants to actually be old?
- We then address the issue of how to define successful aging. The term success implies some sort of normative judgement on desirable and undesirable end states. This raises two questions: What can be considered as a meaningful end state of development? And which criteria should be employed to evaluate the desirability of those end states? We review the state of research on these questions and existing attempts to define successful aging in the second part of this research paper.
- In the final part of this research paper, we discuss some of the current models of developmental regulation in old and very old age. These models shift the focus from a criteriaoriented approach addressing the question What is successful aging? to a more process-oriented approach addressing the question How do people age successfully? These models underscore that motivational processes of setting, pursuing, and maintaining personal goals are of central importance for understanding how individuals manage to age well.
Characteristics of Old Age
When is a person considered to be old? Old age, the final phase in life, is commonly thought to begin somewhere between the ages of 60 and 70. An often cited (somewhat arbitrary) threshold is the age of 65. For employees, retirement represents a cultural marker of entering old age. Many people in their 60s, however, appear still young, whereas others have apparently been old for quite some time. Chronological age does not tell much about a person’s biological (e.g., functional capacity), psychological (e.g., feelings, attitudes, interests, future perspectives), or social age (e.g., life activities, occupied roles; see Aiken, 1989).
Even within a given person, aging is no uniform process. Different organs, organ systems, and capacities in various functional and psychological domains show differential patterns and rates of aging (P. B. Baltes, 1989). For example, the reproductive system usually ages more rapidly than the nervous system. Furthermore, other variables—such as poor nutrition, illness, or disuse of abilities—affect the rate and degree of aging-related decline (e.g., Aiken, 1989; Krauss Whitbourne, 1985).
In other words, old age—like any other phase in life—is characterized by tremendous inter- and intraindividual variability. In the subsequent sections we delineate some developments that represent general characteristics of old age.Aging is a very complex process, and it is beyond the scope of this research paper to attempt a comprehensive characterization of that life phase (for a recent overview, see P. B. Baltes, Staudinger, & Lindenberger, 1999).After characterizing aging as a young phenomenon, so to speak, we restrict our discussion to four domains of functioning in which age-related changes are partly considered losses threatening positive functioning in old age: (a) physiological and health-related changes, (b) cognitive abilities, (c) social relationships, and (d) everyday competence.
Old Age Is Still Young
Until relatively recently in human history, only a small proportion of people survived long enough to become old in today’s sense (see Vaupel, 1995): Throughout human history up to about the beginning of the nineteenth century, life expectancy at birth (i.e., the average life span of persons born in a given year) was low for most populations—namely, only between 20 and 30 years. This was largely so because a large proportion of newborns (about one third to one half) died before reaching the age of 5 years. Even for children surviving to age 5, the expected remaining lifetime was only 30–40 years. Only a small minority of people survived diseases, wars, and other life-threatening dangers to become 50. Even for them, the remaining life expectancy was only about 10–15 years.
During the 19th century, life expectancy slowly began to increase. In Finland, for example, where reliable statistics on mortality going back to that time are available (Kannisto, Turpeinen, & Nieminen, 1999), life expectancy at birth increased from 30.4 years for men and 33.2 years for women born between 1801 and 1810 to 45.3 years for men and 48.2 years for women born 100 years later (i.e., between 1901 and 1910). Because of technological advances coupled with improvements in nutrition, sanitation, public health care, and so on, this increase in life expectancy further accelerated during the twentieth century. Men and women born in Finland between 1946 and 1950, for example, had a life expectancy of 58.4 years and 65.8 years, respectively. Estimated life expectancy for children born in Finland another 50 years later (between 1991 and 1995) further increased to 72.1 years (male) and 79.7 (female).
Prior to 1950, the increase in life expectancy largely resulted from reductions in death rates at younger ages— particularly reductions in infant mortality (i.e., from the fact that more people survived to older ages; Vaupel, 1995). The continuing growth of life expectancy since 1950, in contrast, is attributable to the fact that older people live longer. In most modern industrialized countries, death rates above the age of 60 have substantially declined since 1950. This decline has even accelerated—especially since 1970. For example, in modern industrialized countries in 1990, there were about twice as many people in their 90s and four to five times as many centenarians as there would have been if mortality rates after age 80 had stayed the same as in 1960 (Vaupel et al., 1998). To date, the lengthening of the human life span is no longer restricted to modern industrialized countries. More recently, developing countries have started to show similar increases in life expectancy (Meeks, Nickols, & Sweaney, 1999; World Health Organization, 1998). It has been estimated that by the year 2025, 72% of the world’s population aged 60 years and above will be living in developing countries (United Nations, 1996).
In most (particularly in industrialized) countries, the increase in life expectancy has been co-occurring with a decline in fertility rates (i.e., a decrease in the average number of children per woman in childbearing age). Both trends together (i.e., declining mortality and fertility rates) have drastically altered the population’s composition—with the growth of the older population outpacing the total population’s growth. This trend is expected to continue in the future, with the fastest expanding group being the oldest old (Dinkel, 1994). Prognoses of the World Health Organization (1998), for example, predict that in Europe’s population, the proportion of people older than 60 will increase from about 20% at the end of the twentieth century to about 25% by the year 2020. Estimates indicate that by 2020, the proportion of people older than 80 years in the age group above 60 will make up 22% in Greece and Italy; 21% in Japan, France, and Spain; and 20% in Germany (World Health Organization, 1998).
This lengthening of the average human life might be viewed by many as one of the most precious achievements in recent human history. It does, however, also pose new challenges to cultural and societal developments. Societies need to develop policies that ensure—despite declining proportions of working-age people—adequate income, housing, health care, and other living conditions that provide opportunities for an independent, integrated life for the growing number of older people (United Nations, 1996). To meet this challenge, gerontology needs to seek knowledge about conditions promoting positive aging and to give answers to such questions as what represents adequate housing for the elderly and how to support independent living in old age. This is one of the reasons that the topic of successful aging is not only of scientific but also of social and political importance.
Paradoxically, in one sense old age is a young phenomenon. To date, not much is known about this life phase in general or about processes and conditions that promote successful aging in particular. As a first step in approaching the topic of successful aging, we briefly outline the specific conditions of old age. We start by giving a very short overview of the physiological and health-related changes in old age.
Physiological and Health-Related Changes in Old Age
Aging is characterized by physiological changes that lead to progressive structural and functional decrements in all tissues and organs (for overviews, see Aiken, 1989; Whitbourne, 1985; Medina, 1996). Most obvious to the lay observer are typical changes in appearance—for example, aging skin; graying or whitening hair; changes in body shape and stature; decreased muscular strength and endurance; increased stiffness in the joints; and a general slowing, increased sway, and insecurity while walking or performing motor tasks. Aging is also accompanied by impairments in the functioning of all the sense organs—vision, hearing, taste, smell, vestibular senses (necessary for the maintenance of posture and balance), and sensitivity to touch, pain, and temperature (i.e., cutaneous senses). Sensations become increasingly dull, and responses to sensory stimuli slow down with age. Physiological aging is also characterized by a gradual deterioration of internal organs, leading to a reduced efficiency of the body’s vital systems. Age-associated changes in the various systems generally interact. Cardiovascular functions, for example, are influenced by age-associated changes in respiratory function, which in turn are influenced by changes in the musculoskeletal system (Steinhagen-Thiessen, Gerok, & Borchelt, 1994).
Overall, the physiological changes accompanying aging result in reduced functional capacity, impaired biological resilience in the face of stress, lessened ability to physiologically adapt to environmental changes, prolonged phases necessary to physically recuperate from strenuous effort, and—most important—increased susceptibility to acute and chronic diseases (Aiken, 1989; Steinhagen-Thiessen et al., 1994). It is therefore not always possible to clearly delineate normal physiological aging and pathological changes.
Although age-associated physiological changes are inevitable, they represent no uniform biological process. The kind and magnitude of age-related changes vary greatly from individual to individual. Furthermore, physiological changes interact, for example, with psychological, social, environmental, and lifestyle factors to determine the course and rapidity of aging (Fries, 1990; Rowe & Kahn, 1987; Siegler & Costa, 1985). For example, attitudes and personality characteristics may influence the degree to which an old person seeks intellectual stimulation or engages in physical or social activities, which in turn decelerate and attenuate decline in relevant functional domains. On the other hand, reduced mobility due to physiological impairment might obstruct such activities, precipitating further decline (Bortz, 1982). In this sense, physiological decline associated with aging is not entirely uncontrollable. Particularly lifestyle habits, such as regular exercise, balanced nutrition, and social and intellectual stimulation through active participation might at least temporarily postpone or attenuate physiological decrements associated with aging (Fries, 1990).
In short, physiological changes accompanying aging result in a reduction of the organism’s functional capacity and an increased vulnerability to chronic and acute illnesses. These detrimental effects of physiological aging become particularly pronounced in very old age (85 years and beyond). Although it is unavoidable, physiological aging is no uniform progress. It is in part determined by lifestyle factors and thus—particularly in young-old age—temporarily and within boundaries modifiable.
Cognitive Abilities in Old Age
A popular view on aging is that cognitive abilities drastically decline with age (e.g., Heckhausen, Dixon, & Baltes, 1989). Old people are expected to become more and more forgetful, to have large difficulties understanding new things, and to not think as clearly as younger persons. On the other hand, wisdom, life experience, or professional expertise in their commonsensical understanding are clearly positively associated with old age (Clayton & Birren, 1980; Sternberg, 1990). What has science revealed about cognitive aging?
Building on the recognition that cognitive functioning is influenced by biological as well as cultural processes, research has distinguished two main categories of intellectual abilities—the mechanics and pragmatics of cognition (P. B. Baltes, 1987; P. B. Baltes, Lindenberger, & Staudinger, 1998; P. B. Baltesetal., 1999). This distinction draws on and extends earlier conceptualizations, such as the theory of fluid and crystallized intelligence by Cattell and Horn (Cattell, 1971; Horn, 1982). The mechanics of cognition stand as metaphor for the largely neurophysiological basis of cognition as it evolved during biological evolution. They represent the hardware of the mind, so to speak, and become evident in the speed, accuracy, and coordination of basic information-processing operations. The pragmatics of cognition, in contrast, comprise the culturally transmitted bodies of knowledge individuals acquire in the course of their socialization. They stand for the software of the mind. Typical examples of pragmatic abilities include reading, writing, language, or professional skills. Delineating mechanics and pragmatics of cognitive functioning does not imply that these represent abilities independent of or exclusive from each other. Rather, mechanics and pragmatics are assumed to determine intellectual functioning in their interaction: There would not be pragmatics without mechanics and vice versa—mechanics without pragmatics would lack the very medium in which to unfold.
How do these two components of intellectual functioning develop across the life span into old age? Empirical evidence shows that the cognitive mechanics (e.g., memory, processing speed) show a pattern of rapid growth during infancy and childhood into adolescence, a monotonic and roughly linear decline during adulthood, and a further acceleration of decline in very old age (e.g., Case, 1985; Kail, 1991; Kail & Salthouse, 1994; Lindenberger & Reischies, 1999; Schaie, 1994, 1996).
This trajectory of loss in the cognitive mechanics can be counteracted to some degree by specific training. Training studies have shown that the majority of healthy older adults are able to improve their performance in tasks reflecting mechanic abilities during training (e.g., P. B. Baltes, Sowarka, & Kliegl, 1989; P. B. Baltes & Willis, 1982; Hayslip, 1989; Kliegl, Smith, & Baltes, 1990; Schaie & Willis, 1986; Verhaegen, Marcoen, & Goossens, 1992). Those training gains, however, are highly task-specific. Transfer to related abilities or generalization to everyday functioning is unlikely (P. B. Baltes, Dittmann-Kohli, & Kliegl, 1986; P. B. Baltes & Lindenberger, 1988). Moreover, the amount of plasticity (i.e., the range of potential change) in the cognitive mechanics clearly decreases with age (e.g., P. B. Baltes & Kliegl, 1992; Singer, 2000).
Pragmatic abilities show a more favorable life-span trajectory than the mechanics do. They remain stable or increase well into young old age (i.e., up to about 75 years of age), and only after that show some decline, which is much less pronounced than the decline in the cognitive mechanics (e.g., skill-specific expertise: Bosman & Charness, 1996; Charness, 1981a, 1983; Knopf, Kolodziej, & Preussler, 1990; wisdom: P. B. Baltes, Staudinger, Maercker, & Smith, 1995; Clayton & Birren, 1980; Staudinger, 1996; complexity and differentiation of self-representation: Labouvie-Vief, Chiodo, Goguen, Diehl, & Orwoll, 1995).
As mentioned before, mechanics and pragmatics conjointly influence cognitive performance in all age groups. Particularly important for understanding the development of cognitive abilities in old age are two observations:
- Up to a certain threshold in impairment of the cognitive mechanics, pragmatic knowledge can be efficiently utilized to compensate for age-based losses in mechanics. Evidence for this has been provided by quasi-experimental studies on age- and skill-related differences in chess (e.g., Charness, 1981a, 1981b), bridge (e.g., Charness, 1983, 1987), and transcription typing (e.g., Bosman, 1993; Salthouse, 1984; Salthouse & Saults, 1987). A classic illustration is a study on aging typists (Salthouse, 1984); in this study, age was negatively related to typing speed but positively related to eye-hand span. Older typists might have compensated the slowing of their typing (as an expression of cognitive mechanics) by looking further ahead in the to-be-typed text (i.e., a strategy pertaining to knowledgebased pragmatics). The idea that the knowledge-based pragmatics efficiently compensate mechanic decline in older adulthood is further supported by the finding that compared to standard psychometric assessments using artificial and isolated cognitive tasks, negative age trajectories tend to be attenuated in familiar (i.e., knowledgerelevant) domains with everyday relevance, such as everyday problem solving (e.g., Berg & Klaszynski, 1996; Willis, 1996) or memory in context (e.g., Hess & Pullen, 1996).
- If, however, the mechanic information-processing capabilities fall below some critical threshold, they delimit the overall capability of cognitive integrity and consequently also impair intellectual functioning in the pragmatic domain (P. B. Baltes, 1997). Individuals reaching a very advanced age are therefore particularly vulnerable to reach such levels of impairment in mechanic abilities that intellectual functioning in a more global manner is substantially impaired. Indeed, correlations among abilities both between and within the cognitive pragmatics and mechanics are higher in very old adults than in younger or middleaged adults (for an overview, see Li & Lindenberger, 1999). This dedifferentiation in very old age appears to transcend the cognitive domain and to also affect sensory and sensorimotor functioning (e.g., Anstey, Lord, & Williams, 1997; Lindenberger & Reischies, 1999; Salthouse, Hancock, Meinz, & Hambrick, 1996). These findings point to the impact of domain-general processing constraints in very old age, which is further illustrated by the empirical observation that in very old age, the differences in the directionality of the development of pragmatic and mechanic abilities seem to disappear and to give way to negative age-gradients in both domains (Lindenberger & Reischies, 1999).
In sum, there is evidence for age-related decline in the biologically based cognitive mechanics. At least up to a certain point, this development can be compensated by culturally determined, knowledge-based cognitive pragmatics. Most older adults are cognitively well able to manage everyday life problems. In very advanced old age, however, a somewhat different picture emerges. Here, the cognitive mechanics might reach a level of impairment that the efficiency of intellectual functioning declines in a more global manner. This development is also reflected if we take a look at pathological cognitive changes in old age. The prevalence of dementias increases steeply with age. Several studies have observed that in adults above the age of 60, age-specific prevalence rates of dementias almost double with each additional 5 years of age, leading to prevalence estimates of more than 40% in the population aged 90 years and beyond (e.g., Cooper, 1997; Hofman et al., 1991; Jorm, Korten, & Henderson, 1987).
Social Relationships in Old Age
Kahn and Antonucci (Antonucci, 1985, 1990, 1991; Kahn & Antonucci, 1980) coined the metaphor of social convoys to express the idea that throughout their lives, people are surrounded by significant other persons who have a critical influence on their lives. Social integration has been shown to have a significant beneficial impact upon a person’s well-being (e.g.,Antonucci &Akiyama, 1995; Bowling, 1994; Brubaker, 1990; Kessler & McLeod, 1985), health (e.g., Antonucci & Jackson, 1987; Lang & Carstensen, 1998; Schwarzer & Leppin, 1991), and even mortality (e.g., Seeman, 1996; Tucker, Schwartz, Clark, & Friedman, 1999). Social contact, however, may also have its negative sides. Such experiences include undesirable, ineffective, or excessive support; unpleasant or overly demanding social contact; violence or neglect; and anticipated or experienced loss of social partners (Lang & Carstensen, 1998; Smith & Goodnow, 1999).
As people grow older, their relationships and social networks undergo considerable change not only as a result of changing contexts (e.g., retirement, one’s own or others’ disease and frailty, grandparenthood, relocation, deaths of significant others) but also as a result of changes in the individual’s behaviors and pBibliography: (Lang & Carstensen, 1998). In any event, interpersonal contexts in old age remain multifaceted and heterogeneous. Social networks of older people who are widowed, have never married, or are childless, for example, differ in many respects from those who are living with their partner or are highly involved in the families of their children.
Typically, the number of social contacts declines with advancing age (e.g., Heller & Mansbach, 1984; Lang & Carstensen, 1994; Palmore, 1981). Investigations in the United States and Europe indicate that older people above age 65 typically report having between 5 and 15 close social partners in their social networks compared to a range from 15 to 35 network members in the social networks reported by younger and middle-aged adults (e.g., Antonucci & Akiyama, 1994, 1995; Dykstra, 1993; Lang & Carstensen, 1994, 1998; van Sonderen, Ormel, Brilman, & van Linden van den Heuvell, 1990). As we elaborate when discussing socioemotional selectivity theory later in this research paper, it is questionable whether this decline indeed constitutes a developmental loss as it might appear at first glance (Carstensen, 1993).
Functions of social relationships can be characterized by three main themes—support, affectionate exchanges, and socializing (i.e., interacting with visitors and engaging in shared activities; e.g., Antonucci & Akiyama, 1995; Wagner, Schütze, & Lang, 1999). Generally, the proportion of network partners from whom emotional or instrumental help is received increases with age because of aging-related increases in frailty (e.g., Mares, 1995; Zarit & Eggebeen, 1995). Old and even very old persons, however, typically also give support, but not to the same degree (e.g., Antonucci, 1991; Zarit & Eggebeen, 1995). Although social support relationships gain in significance with advancing age, socializing and affect exchange remain important functions of social contact. In a sample of German older persons, for example, the number of people with whom participants socialized and with whom they were affectionate decreased into very old age; yet the proportions within the network (around 30% and 20% of the social partners, respectively) did not (Wagner et al., 1999).
Historical increases in life expectancy have led to an increase in the length of marital relationships among those who do not divorce. These demographic developments have also increased the average duration that is spent in illness or caregiving before the relationship is eventually ended by the death of one partner. Because women at any given age have a longer life expectancy than men have and also tend to marry men who are somewhat older, they are more likely to be caretakers of ailing husbands, are more likely to survive husbands than to be survived, and tend to spend a larger proportion of their life spans following the death of a spouse (Bradsher, 1997).
The death of one’s partner is undoubtedly one of the most disruptive losses that an individual can be confronted with in life. In addition to the immense grief over the loss of a loved person, bereavement often brings with it significant changes and losses in everyday tasks and routines, economic or social status, and even personal self-identity (Bradsher, 1997). The most impressive evidence of the extreme mental and physical suffering associated with losing a loved one is the wellreplicated observation that bereaved persons (particularly men) have a higher mortality risk than do matched samples of nonbereaved controls, especially in the weeks and months immediately following the loss (Stroebe & Stroebe, 1993). The vast majority of elderly people, however, eventually adapt to their dramatically changed life situation within the first few years, as indicated by significant reductions of psychological distress and improvements of mental health and well-being back to levels comparable to those before the loss (e.g., Gallagher-Thompson, Futterman, Farberow, Thompson, & Peterson, 1993; Lund, Caserta, & Dimond, 1993).
Particularly after the loss or in the absence of other relationships, contact between siblings often gains in closeness in late life (Cicirelli, 1985; Connidis, 1989; Scott, 1983). As people grow old, their family of origin gradually disintegrates because its older members die. Sibling relations represent the most enduring ties of the original nuclear family (Cicirelli, 1985). Their most significant function in late life seems to be reminiscence about shared experiences in “good old times.” It has been argued that the validation of positive feelings in previous family interactions may be related to positive feelings about the family in later life (Brubaker, 1990). The role of siblings in providing instrumental support is comparatively less important (Goetting, 1986)—especially when sibling support is compared to assistance provided by adult children (Cicirelli, 1982; Ross & Milgram, 1982; Scott, 1983), who are frequently important sources of emotional and instrumental support in old age (for overviews, see Antonucci & Akiyama, 1995; Brubaker, 1990; Lang & Carstensen, 1998; Mares, 1995; Zarit & Eggebeen, 1995).
Friends also often play a central role in older people’s social lives (Field, 1999; Wagner et al., 1999). They are, however, typically less important than family to old persons. De Vries (1996) argued that later life is a phase with a particularly high likelihood of life events that might influence the maintenance of friendships—for example, retirement, relocation, or illness. Particularly for men, retirement often is associated with a relatively high risk of erosion of work-based friendships. Female friendships that originated in work contexts are typically more broadly based and thus less prone to dissolution after retirement. Relocation (e.g., moving closer to one’s children or into a nursing home) may also affect the maintenance of later life friendships. At the same time, it might provide opportunities for forming new friendships, an ability that is preserved well into old age (M. M. Baltes, Wahl, & Reichert, 1991; Field, 1999). The most important barriers to friendship contact in late life, at least for older persons living in private households, are one’s own or the friend’s illness and frailty. Furthermore, the likelihood of outliving one’s friends increases with age; this is reflected by observations in a sample of German older persons. Sixtynine percent of the 70- to 84-year-old participants reported having at least one friend, compared to 43% of the (more frail) participants aged 85 years and over (Wagner et al., 1999).
To summarize, the majority of old people are well integrated into their family and friendship networks. Overall, the size of social networks declines with advancing age. The decline in network size is typically due to a decrease in social contact with emotionally not-very-close network partners. Contact with emotionally close persons—particularly with family, but also with some close friends—stays relatively stable. With increasing frailty or disability, support provided by network partners gains in importance. Even in very old age, however, support is not only received but also (at least to some degree) given. Socializing and exchange of affection also remain important into very old age. Social contact with same-aged persons in old age is characterized by an increasing likelihood that one’s own or the other’s frailty obstructs possibilities for maintaining the relationship in habitual ways. Also, the risk increases that relationships are ended through the deaths of social partners, one of the most hurtful experiences in the social lives of human beings. Most old adults, however, are able to successfully cope with the experience of outliving peers.
Everyday Competence in Old Age
So far we have discussed characteristics of aging pertaining to a selected number of clearly circumscribed functional domains—health-related and physiological changes, cognitive abilities, and social relationships. Those and other domainspecific characteristics of old age converge in an overarching question: How well are old adults able to care for themselves, manage their affairs, and live an autonomous life?
The ability to perform activities essential for the effective mastery of independent living has been referred to as everyday competence (e.g., M. M. Baltes, Mayr, Borchelt, Maas, & Wilms, 1993; Diehl, 1998; Schaie & Willis, 1999). M. M. Baltes and colleagues (M. M. Baltes, Maas, Wilms, Borchelt, & Little, 1999; M. M. Baltes et al., 1993; M. M. Baltes & Wilms, 1995) distinguished two components—a basic and an expanded level of competence. According to M. M. Baltes and colleagues, the interplay of both components makes up the ability to lead an autonomous and satisfying life. The basic level of everyday competence reflects the ability to independently execute personal maintenance activities, such as toileting, grooming, dressing, walking, or shopping; these are highly routinized activities necessary for survival. The expanded level of everyday competence comprises activities that reflect people’s active construction of their lives, their pBibliography: and motivations, and their engagement with the world around them. Examples are engaging in leisure, outof-house, or social activities; helping others; and working. Whereas the basic level of competence guarantees survival, it is the expanded level that turns mere existence into meaningful living.
The Basic Level of Everyday Competence in Old Age
In clinical terms, the basic level of competence reflects an individual’s functional health or disability, which is typically assessed by evaluating the degree of help needed for the execution of basic and instrumental activities of daily living (referred to as ADL and IADL; Katz, Ford, Moskowitz, Jackson, & Jaffe, 1963; Lawton & Brody, 1969). The need for assistance in the management of everyday life has been shown to be determined primarily by impairments in the sensory, sensorimotor, and motor domains (e.g., M. M. Baltes et al., 1999; Steinhagen-Thiessen & Borchelt, 1999; see also Diehl, 1998), as well as by functional impairment in the cognitive domain (for summaries, see Diehl, 1998; Willis, 1996). The main risk factor for such functional impairments is somatic morbidity. Different illnesses, however, differentially influence a person’s ability to engage in independent living (Furner, Rudberg, & Cassel, 1995). Boult, Kane, Louis, Boult, and McCaffrey (1994), for example, reported that the chronic conditions best predicting the development of dependence in ADL and IADL were cerebrovascular disease, arthritis, and coronary artery disease.
Several studies in modern, industrialized countries have observed that the ongoing decrease in mortality rates in old and very old age coincides with a decline in chronic disability prevalence in that age group (i.e., a decline in the proportion of elderly people with long-term dependence on help for the execution of at least one ADL or IADL; e.g., Bebbington, 1988; Jagger, Clarke, & Clarke, 1991; Manton, Corder, & Stallard, 1993). Manton et al. (1993), for example, reported that whereas the total U.S. population above age 65 grew 14.7% between the years 1982 and 1989, the respective proportion of chronically disabled community-dwelling and institutionalized persons only grew 9.2%. Consequently, the overall prevalence (i.e., relative proportion) of chronic disability or institutionalization dropped from 23.7% in 1982 to 22.6% in 1989. The decrease in chronic disability prevalence in developed countries has been attributed primarily to advances in medical treatments and—to some degree—to increases of the average education and income in elderly cohorts, which are typically associated with an increased self-awareness of health-related lifestyle factors and an early use of professional prevention and therapy (Manton et al., 1993).
Originally developed in the context of mortality developments in old age, the concept of active life expectancy addresses the basic level of everyday competence in the temporal dimension of an individual’s expected remaining lifetime. Active life expectancy represents the period of life an individual is expected to be able to perform functions necessary for personal care and independent living. Inactive life expectancy, in contrast, represents the remaining lifetime when one is unable to perform these functions or would be dependent upon others to perform them (Crimmins, Hayward, & Saito, 1996).
Significant differences in active life expectancy exist with respect to gender, age, and socioeconomic status (SES). A well-known paradox of the aging process is that women tend to live longer, yet they have a higher prevalence of disability (i.e., dependence) than do men (Verbrugge, 1989). Crimmins et al. (1996), for example, reported the total remaining life expectancy for U.S. females at age 70 to be 13.9 years and for same-aged U.S. males to be 10.3 years. The expected length of life in an inactive state, however, was twice as high for 70-year-old women (2.8 years or 20.1% of remaining expected lifetime) as that for same-aged men (1.4 years or 13.6% of remaining expected lifetime). Gender differences in the diseases that cause disability play a role in the explanation of this paradox. Women have a higher prevalence of more slowly evolving degenerative processes (e.g., arthritis, skeletal problems, diabetes), whereas men are more at risk to suffer (and die) from more rapidly developing lethal diseases (e.g., cancer, heart attack; Manton, 1990). Overall, women have a higher risk of experiencing longer phases of inactive life, a greater likelihood of experiencing disabling events (i.e., the transition from independent to dependent life), and a greater likelihood of dying from a disabled state (Crimmins et al., 1996).
The percentage of remaining life time expected to be spent in dependent states is higher at any age above 70 for women, but for both sexes it increases rapidly with age. Crimmins et al. (1996), for example, reported for U.S. women an increase from 20.1% at age 70 to 60.4% at age 90. The corresponding estimates for U.S. males increased from 13.6% at age 70 to 54.5% at age 90. On the other hand, there is a great variability regarding independent living among old adults. Even in very old age, quite a few individuals exhibit a high degree of independence. In a study of 109 Italian centenarians (aged 100–108 years), for example, 26% of the participants (34.6% of the male and 24.0% of the female centenarians) were classified as completely independent in basic activities of daily living (Bauco et al., 1996).
In addition to gender and age, SES also is associated with basic levels of everyday competence. Those of higher SES are not only more likely to survive to old age, but they are also more likely to live through old age in better functional health (e.g., Feldman, Makuc, Kleinman, & Huntley, 1989; Maddox & Clark, 1992; Matthews, Kelsey, Meilahn, Kuller, & Wing, 1989). In the representative sample of U.S. older persons investigated by Crimmins et al. (1996), active life expectancy for persons with at least 12 years of education was about 1 year longer than that of persons of same age, race, and sex with less education.
The Expanded Level of Everyday Competence in Old Age
How do older adults structure their daily lives above and beyond activities necessary for self-maintenance and survival? Detailed reconstructions of a complete day in the lives of older Germans (M. M. Baltes et al., 1999; Horgas, Wilms, & Baltes, 1998) indicated that on average, 60% of the waking day was spent on activities that were not resting and not selfcare. Although there was a substantial amount of variability in the amount of time spent with discretionary activities (Horgas et al., 1998), it appeared that a large amount of time was typically spent on leisure activities (mostly watching TV; about 38%) and on instrumental activities (e.g., housework, dealing with authorities, banking; about 15%). Only 7% of the waking day were on average spent on social activities. The oldest old (aged 85 years and above) as well as institutionalized participants tended to spend less time with instrumental and leisure activities and more time resting compared to young old (aged 70–84 years) and noninstitutionalized participants. Women tended to spend more of their waking time on instrumental activities and less time on leisure activities than did men, which reflects the culturally typical housework distribution in that age group.
- M. Baltes and colleagues (M. M. Baltes et al., 1999) observed that the level of expanded everyday competence (i.e., the degree of engagement in activities other than selfcare and resting) was substantially negatively related to chronological age and substantially positively related to SES. Both relationships were completely mediated by personality characteristics, fluid intelligence, and mobility. Thus, age differences in expanded levels of everyday competence seem to be due to associated differences in health and psychosocial factors. Furthermore, psychosocial resources such as education, financial security, and openness to experience appear to be necessary to guarantee high levels of involvement in discretionary activities. They are, however, not sufficient. Activities indicative of expanded everyday competence also require a critical level of physiological functioning.
In sum, there is great variability in old adults’ abilities to lead independent, meaningful, and satisfying lives. Basic levels of everyday competence (i.e., the ability to independently execute activities necessary for self-maintenance and survival) largely depend on the level of functional impairment in sensory, sensorimotor, motor, and cognitive domains. In contrast, the expanded level of competence (i.e., the degree of involvement in discretionary activities that make a life meaningful) is largely determined by psychosocial variables—particularly personality characteristics and cognitive abilities, but it also requires a minimum level of functional health. With advancing age, levels of basic and expanded everyday competence tend to decline, which is due to age-associated changes in physical morbidity and psychosocial variables.
Conclusions: What Characterizes Old Age?
We have characterized the life phase of old age in four relatively well-specified life domains—physiological changes, cognitive functioning, social relations, and everyday competence. On a more abstract level, three central characteristics of old adulthood can be inferred from this discussion:
- With advancing old age, the likelihood of developmental losses increases (e.g., development of chronic and acute illnesses, impairment in the cognitive mechanics, deaths of social partners, loss of the ability to lead an independent life). Overall, the ratio of developmental gains and losses becomes increasingly negative in old age.
- Aging is no uniform process. A large degree of heterogeneity exists both among and within persons. Different functional domains are differentially affected by aging processes.
- Old adults in their 60s and 70s typically exhibit relatively high levels of functioning in different life domains. In very old age (85 years and older), however, detrimental effects of aging become more pronounced. It is therefore necessary to differentiate between a young-old and an older- or oldest-old age.
After having portrayed characteristics of old age in general, we next turn to the question of if and how one can characterize successful aging. Following that discussion, we review a number of theoretical approaches to developmental regulatory processes in old age.
Successfulaging: Definition and Criteria
For several decades, gerontology has struggled to understand and define what successful aging is. As of yet, however, no commonly accepted set of criteria characterizing successful agingexists.Ingeneral,therehasbeenashiftawayfromdefining successful aging solely in terms of adaptation to agerelated changes in a given context (e.g., Havighurst, 1963) toward emphasizing the balance between a person’s needs and competence on the one hand and environmental demands and opportunity structures on the other hand (Lawton & Nahemow, 1973; Thomae, 1976). In accordance with life-span developmental approaches (e.g., P. B. Baltesetal., 1998; Brandtstädter, 1998; Lerner, 1998; Lerner & Busch-Rossnagel, 1981; Magnusson, 1996), these newer conceptualizations of successful aging assume that development is best described as an ongoing and dynamic interaction of a person with his or her environment. This implies that criteria of successful aging should not exclusively comprise factors within the person (e.g., happiness), but should also consider how well a person is doing in a given context (e.g., living in a nursing home).
Attempts to define criteria of how well a person is aging have—at least on a theoretical level—also shifted from a one-criterion approach (mostly using subjective well-being as the only criterion signaling successful aging) to a multicriteria approach. The multiple criteria that have been proposed as characterizing successful aging comprise objective and subjective, short-term and long-term, domain-specific and general, and static and dynamic criteria (M. M. Baltes & Carstensen, 1996; P. B. Baltes & Baltes, 1990). Thus far, however, no consensus has been reached on the questions of which of these criteria have to be met and what their relative importance for determining successful aging is.
Based on the assumption that adaptation to challenges specific to old age and a successful person-environment interaction results in subjective well-being (e.g., Havighurst, 1963; Lawton, 1989), most research on successful aging has employed subjective well-being as a single criterion for successful aging. Next, we provide a brief overview of the empirical evidence available on subjective well-being in old age. Then we turn to a discussion of more comprehensive conceptualizations proposing multiple criteria for the characterization of successful aging.
Is Subjective Well-Being a Sufficient Criterion for Successful Aging?
The most prominent single criterion that has been used for studying successful aging has been subjective well-being. In this line of research, subjective well-being is viewed as a person’s global evaluation of the quality of his or her life. High subjective well-being is regarded as indicating that the person successfully manages his or her life and ages well.
Subjective well-being is operationalized most often in terms of life satisfaction, the presence of positive affect, and the absence of negative affect (e.g., Diener, Suh, Lucas, & Smith, 1999). Bradburn (1969) limited subjective well-being to the affective reactions towards one’s life experiences. More specifically, he defined happiness as a preponderance of positive over negative affect. Life satisfaction, on the other hand, focuses on the cognitive assessment of progress towards or achievement of one’s goals (Campbell, Converse, & Rodgers, 1976; George, 1981; Lawton, 1985).
Both the cognitive and affective aspects of subjective well-being have been widely studied in gerontology. The central question motivating this line of gerontological research is Does subjective well-being decline with age? An assumption underlying this question is that subjective well-being is threatened in old age (e.g., Brandtstädter & Greve, 1994). The expectation of an age-related decline in subjective wellbeing is based on the observation that old age is a period in life when one is more likely than in earlier phases to experience severe losses: Most old people are excluded from productive employment, almost everybody in this age-group experiences a decline in physical capacity and health (e.g., Steinhagen-Thiessen & Borchelt, 1999), and old people are likely to lose close social partners (e.g., Lang & Carstensen, 1994). We have described a number of these developmental losses associated with aging in more detail in the first part of this research paper. There also is much consensus in social expectations that old age is related to losses rather than gains (Heckhausen et al., 1989). Wouldn’t one then expect older people to be dissatisfied with their lives and unhappy? In the following section, we briefly review the literature on emotional well-being and life satisfaction in old age.
With regard to age-related changes in the experience of emotions, Schulz (1986) suggested that because of lifelong experiences, older persons should be habituated to emotions and hence have a higher threshold for experiencing both positive and negative affect. This should lead to less frequent but more intense emotions. Emotions might also linger for a longer time because autonomous activation takes longer to go back to baseline. Contrary to these expectations, Levenson, Carstensen, Friesen, and Ekman (1991) found that the physiological arousal pattern of older adults is comparable to that of younger adult but of less intensity. These results have recently been replicated in a sample of young and older European and Chinese Americans (Tsai, Levenson, & Carstensen, 2000). In this study, older adults showed smaller changes in cardiovascular responding to positive (amusement) and negative (sadness) emotions than did younger adults. Young and old adults did not, however, differ in their self-reported and behavioral expression of emotions during standardized situations (watching film clips). Using a different methodology—namely, selfreported intensity of emotions—Ferring and Filipp (1995) found that the self-rated intensity of general positive emotions seems to decline with age, whereas the intensity of general negative emotions did not appear to be age-related.
With regard to old and very old age, findings from the cross-sectional data set of the Berlin Aging Study (Smith, Fleeson, Geiselmann, Settersten, & Kunzmann, 1999) suggest that within the three decades from 70 to 100 years, chronological age is not or is only weakly associated with the self-reported frequency of affect. Although with increasing age, self-rated frequency of positive affect tended to decrease somewhat (r .22), there was no significant correlation of age with frequency of negative affect. In a longitudinal study, Ferring and Filipp (1995) found that with increasing age, older adults reported less frequent positive and more frequent negative emotions. Lawton, Kleban, and Dean (1993), on the other hand, showed that older people reported less frequent depression, anxiety, hostility, and shyness than did younger adults, and—with the exception of contentment—did not differ from younger adults with regard to positive affect frequency.
Evidence from the Duke Longitudinal Study suggests that there are neither cross-sectional nor longitudinal age-related differences in the level of self-reported life satisfaction in middle-aged and older adults (Palmore & Kivett, 1985); this appears to be also true in very old age. Data from the Berlin Aging Study showed only a small negative correlation of age and satisfaction with aging and no significant correlation of age with life satisfaction (Smith et al., 1999).
The differences in some of the findings reviewed previously (e.g., regarding intensity of emotions) might be due partly to methodological differences (questionnaires vs. physiological assessment), partly to the specific age range of the samples under study, and partly to differences between longitudinal and cross-sectional findings. Although some studies suggest that the frequency of positive emotions might decline in old age (Smith et al., 1999; Ferring & Filipp, 1995), the age-related effects are small and the findings are not consistent (e.g., Lawton et al., 1993). Overall, the empirical evidence suggests stability rather than decline in subjective well-being in old age.
This phenomenon—average stability of subjective indicators of well-being in a life phase when people are confronted with loss and decline in both external and internal resources— has been labeled a paradox (e.g., Brandtstädter & Greve, 1994; Staudinger, Marsiske, & Baltes, 1995) and has called for explanations. Labeling this finding a paradox reflects the assumption that age-related losses are detrimental to a person’s well-being; yet research on subjective well-being shows that the presence or absence of favorable living conditions such as wealth or health does not have a strong or long-lasting impact on people’s subjective well-being (see Diener et al., 1999, for a comprehensive review of the literature).
One of the explanations for this counterintuitive finding is that it is change in living conditions rather than their absolute quality that affects a person’s well-being (Hobfoll, 2001). According to models of hedonic adaptation (e.g., Frederick & Loewenstein, 1999), persons emotionally adapt very quickly to changes in their lives by setting new standards. Even when drastic changes in living conditions occur, such as winning a lottery or encountering an accident causing paraplegia, individuals seem to adapt astonishingly fast when subjective well-being is used as a criterion (Brickman, Coates, & JanoffBulman, 1978).
Consequently, there is no reason to expect that the losses occurring in old age should have a long-term negative effect on older persons’subjective well-being (Carstensen & Freund, 1994). Overall, then, subjective well-being does not appear to be a sufficient criterion signaling successful aging. Newer conceptualizations, therefore, go beyond a single-criterion approach and propose multiple criteria to define successful aging. In the subsequent section, we review the most prominent of these multiple-criteria definitions.
Beyond Well-Being: Other Criteria for Successful Aging
One of the recent attempts to take a more comprehensive approach to characterizing well-being is Ryff’s (1989, 1995) model of positive psychological functioning. Ryff differentiates between six dimensions of positive psychological functioning: autonomy, environmental mastery, personal growth, positive relations, purpose in life, and self-acceptance. Ryff’s model is partly based on subjective conceptions of positive functioning in middle-aged and older adults. Ryff (1989) found that older adults define fulfillment not primarily in terms of positive emotions, but rather as a sense of accomplishment, enjoyment of life, and caring for others.
Ryff’s approach to defining positive psychological functioning, although it is more comprehensive than focusing exclusively on emotional well-being and life satisfaction, is also a subjective approach because it exclusively relies on older persons’ self-reports. Going even further, P. B. Baltes and Baltes (1990) argued for integrating objective (i.e., observable) and subjective (i.e., self-reported) criteria for defining successful aging. They provided a list of objective and subjective criteria that are most often considered in the literature on successful aging: longevity, physical and mental health, cognitive functioning, social competence, productivity, perceived personal control, and life satisfaction. According to P. B. Baltes and Baltes (1990), integrating objective and subjective criteria is important because on the one hand, considering exclusively subjective criteria (such as selfreported well-being) might lead to a neglect of optimizing environmental conditions that support successful aging. A prescriptive definition specifying exclusively objective criteria for successful aging, on the other hand, is based on the scientific community’s specific value system, which might not be shared by the elderly person. Should an elderly person who encounters health-related problems—as elaborated previously, an almost normative event in old and very old age (e.g., Manton, 1990)—not be considered as aging successfully even if happy and satisfied with his or her life?
Addressing the high prevalence of health-related problems in old age, Rowe and Kahn (1987, 1998) distinguished between successful aging and usual aging. Usual aging refers to being able to function well but also being at risk for disease or disability. Successful aging, on the other hand, denotes “the ability to maintain three key behaviors or characteristics:
- low risk of disease and disease-related disability;
- high mental and physical function; and
- active engagement with life” (Rowe & Kahn, 1998; 38).
Rowe and Kahn pointed out that only the combination of these three characteristics represents successful aging. Riley (1998) criticized this approach by arguing that it neglects social structures as an important aspect supporting successful aging: “Successful aging involves the interplay between lives and the complementary dynamic of structural change . . . What Drs. Rowe and Kahn neglect is the dependence of successful aging upon structural opportunities in schools, offices, nursing homes, families, communities, social networks, and society at large” (p. 151).
Similar criticism was raised against early conceptions of successfulagingbyHavighurst(1963;Havighurst&Albrecht, 1953), who defined successful aging as the adaptation to the specific conditions of old age. Thomae (1976), for instance, stressed the role of the environment when he conceptualized successful aging as the balance between an individual’s needs and competence and the demands of the environment.
The previously discussed approaches do not pay attention to the proactive and agentic role of the older person in interacting with his or her environment. According to Lawton (1989), a person does not simply passively adapt to environmental conditions, but rather proactively shapes his or her environment. Proactive choices (such as moving to planned housing) can have long-term consequences on how well the environment fits personal demands. One of the consequences of a good person-environment fit, according to Lawton, is subjective well-being and life satisfaction. Accordingly, Lawton (1983) proposed to define “the good life” (or in a gerontological context, successful aging) along four independent dimensions, including both subjective and objective criteria in different life domains:
- Perceived life quality (subjective satisfaction with various life domains such as family, friends, housing, etc.).
- Psychological well-being (happiness, optimism, congruence between desired and attained goals).
- Behavioralcompetence(health,motorbehavior,cognition).
- Objective environment (income, living conditions, etc.).
Several aspects in this definition of successful aging are worth pointing out. Note first that perceived life quality is not conceptualized as a global evaluation of one’s life as a whole but rather as a multifaceted concept comprising satisfaction with various life domains. As has been shown, for instance, by Diener (1999), global life satisfaction is not simply the average of one’s satisfaction with different life domains. Global life satisfaction seems to be more of a holistic impression of how well one is doing (maybe taking the current mood as an indicator, as suggested by Schwarz and Strack, 1999) than it is the result of a computation of an aggregate score across several life domains. To propose satisfaction with specific life domains as indicators of successful aging is particularly useful if one is interested in how well an aging person is doing in a specific life domain.
Second, note that psychological well-being in Lawton’s sense is a concept broader than emotional well-being. It includes not only positive emotions (happiness), but also optimism—that is to say, “the global expectation that good things will be plentiful in the future and bad things, scarce” (Peterson, 2000, p. 47). Optimism has been repeatedly shown to be positively associated with a number of variables such as positiveemotions,highperformance,andhealth(seePeterson, 2000, for an overview). According to Seligman (1991), optimism is a generalized expectancy of the controllability of outcomes. Feeling in control of events might lead elderly persons to actually take more control over their lives and proactively shape their environments in a way that matches their needs. In this way, one might say that optimism is a factor contributing to processes promoting successful aging rather than a criterion for defining successful aging.
Third, note that—as in the definition of Rowe and Kahn— health is one of the criteria that Lawton lists for identifying successful aging. Because Lawton, however, considers the interaction of a person with his or her environment as crucial for determining successful aging, impaired or sick older persons nevertheless have the potential to age well. Even sick or impaired older persons can successfully interact with their environment by modifying their environment, their activities, or both (i.e., environmental proactivity), thereby enhancing the person-environment fit. Lawton introduces the notion of “control centers,” denoting that disabled older persons may maintain a sense of control by creating an immediate environment in which they can maximize stimulation, knowledge, and security (e.g., by locating a chair in the living room from which they can oversee the street, reach for medicine and books, and keep in contact with the outside by telephone, radio, and TV (Lawton, 1985). In this way, although listing criteria that might imply a static view on successful aging, Lawton’s model of successful aging represents a perspective that focuses on the person-environment interaction.
Taking a similar approach, M. M. Baltes and Carstensen (1996) suggested addressing the problem of defining successful aging by going away from a criteria-oriented approach (which implies the assessment of an end state) to a processoriented approach. Focusing, for instance, on the achievement of long-term goals as a criterion for successful aging as proposed by Lawton, might neglect to consider that goals— whether they will be achieved or not—have a positive function for individuals by organizing and guiding behavior over time and across situations (e.g., Emmons, 1996) and by giving life a purpose (e.g., Klinger, 1977). Because of their function to organize behavior and to contribute to a sense of purpose in life, the very process of having and pursuing personal goals can be viewed as one aspect of successful aging, regardless of the actual achievement of the respective goals.
This perspective adds a new dimension in defining criteria for successful aging—namely, the dimension of a static versus a dynamic approach. According to M. M. Baltes and Carstensen, it is important to assess not only whether an elderly person has achieved positive outcomes (e.g., health, good living conditions, personal goals) but also whether the ongoing process of getting there is one that maximizes gains and minimizes losses—that is, the gains associated with achieving desired outcomes have to be balanced with the costs associated with the outcomes’ attainment (Freund, Li, & Baltes, 1999). Thus, the concept of successful development does not denote a specific end point or state that can be reached but has to take the process of how people achieve desirable states into account. If meeting a certain criterion (e.g., financial security) can only be achieved at high costs (e.g., suffering a number of years in an unfulfilling, boring job), this way of goal pursuit cannot be regarded as being successful (Freund et al., 1999).
A dynamic approach to successful aging also points to another difficult question that has not yet been resolved in the literature—namely, the time window one should best consider when evaluating how successfully an individual is aging. Usually, snapshots of living conditions and well-being of older persons are taken with one-time assessments (cf. Diener et al., 1999). According to a static view on successful aging, such snapshots are sufficient to determine how well older people are doing and what the relationship between living conditions and subjective well-being in older people is at a given point in time. According to a dynamic view on successful aging, however, only multiple assessments in various life domains over time can reveal whether a person interacts with his or her environment in a manner that promotes successful aging in the long run (Freund et al., 1999). For instance, drinking a bottle of wine might help one to relax and feel good in the short run. If continued daily over years, however, the costs of such drinking behavior for physical and mental health are likely to outweigh the short-term gains.
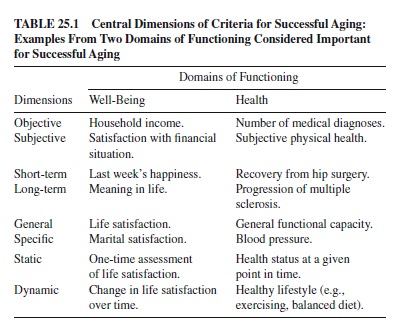
On a very abstract and general level, successful aging can be defined as the simultaneous maximization of gains and minimization of losses. When it comes to differentiating concrete criteria indicating how well a person is aging, however, no generally accepted definition is available. As Pulkkinen (2000, p. 278) stated, “successful development is not uniform but polyform.” Because successful development can take many different expressions, it seems more appropriate to specify criteria depending on the specific research question at hand than to propose a single—necessarily abstract—definition of successful aging. These specific criteria can vary along several dimensions such as objective versus subjective, short-term versus long-term, domain-specific versus general, and static versus dynamic. In Table 25.1, we have summarized these dimensions of criteria for successful aging, giving examples for two life domains that are frequently considered as central to successful aging—namely, well-being and health.
Processes Related to Successful Aging
An alternative route to studying successful aging is to shift the focus away from attempting to define criteria as end points of successful aging to identifying processes of developmental regulation in old age. Although such a processoriented approach does not resolve the question of criteria of successful aging, it redirects the attention to the psychologically interesting question of which developmental processes are central in the interaction of an aging person with his or her environment (M. M. Baltes & Carstensen, 1996). This approach is in line with E. Kahana and B. Kahana’s (1996, p. 25) observation: “The conceptual framework of successful aging is based on the assumption that the aged face unique stresses and challenges. Successful aging requires preventive actions that help delay or minimize normative stresses of aging prior to their occurrence. It also calls for effective corrective actions after older adults encounter normative stresses.” The central question, then, is what processes are involved in minimizing the “normative stresses of aging.” This question lies at the heart of different models of developmental regulation in old age that we discuss next.
We begin by giving some historical background in the form of two models that inspired a lot of theoretical and empirical research activity—namely disengagement theory (Cumming & Henry, 1961) and activity theory (e.g., Maddox, 1963). The debate over whether disengagement is the central process promoting successful aging or whether only those who continue to be actively involved in life are to be considered successfully aging has been largely resolved in newer models (discussed in more detail later in this section), such as socioemotional selectivity theory by Carstensen and colleagues (e.g., 1993, 1995; Carstensen, Isaacowitz, & Charles, 1999).
Successful aging does not appear to be a question of either engagement or disengagement; rather, it is a question of specifying the conditions under which disengagement is more adaptive and the conditions under which activity promotes successful aging. We review three models addressing this question: First, we present a metamodel of successful aging—the model of selection, optimization, and compensation by P. B. Baltes, M. M. Baltes, and colleagues (SOC; e.g., M. M. Baltes & Carstensen, 1996, 1998; P. B. Baltes & Baltes, 1990; P. B. Baltes, 1997; Freund & Baltes, 2000; Freund et al., 1999; Marsiske, Lang, Baltes, & Baltes, 1995). Then we present two models of successful aging that center around the notion of control—namely, the model of primary and secondary control by Heckhausen and Schulz (e.g., 1995) and the model of assimilative and accommodative coping by Brandtstädter and colleagues (e.g., Brandtstädter & Greve, 1994; Brandtstädter & Renner, 1990).
Despite differences among these models, they converge in emphasizing the central role of motivational processes for successful aging. Based on the assumption that a person can take an active part in shaping his or her own development, personal goals (i.e., future states a person desires to attain or wishes to avoid) are seen as playing an important role in a person’s aging process. Personal goals motivate and organize behavior over time and across situations, giving directionality to development. For instance, a person who pursues primarily achievement-related goals might put many hours into practicing golf in order to improve his or her handicap, whereas a person who places more emphasis on affiliationrelated goals might try to spend as much time as possible with his or her friends and family.
Personal goals also serve as a standard of comparison, determining how well a person feels he or she is doing (e.g., Carver & Scheier, 1995). In this sense, the level of aspiration is also associated with subjective well-being—a fact that should be of particular relevance to aging when the likelihood of being confronted with unobtainable or permanently blocked goals is increased. Here, as particularly Brandtstädter and Greve (1994) and Schulz and Heckhausen (1996) argue, adjustment of goal standards should help to protect older persons’well-being. However, as we elaborate in the following discussion, the SOC model, the model of primary and secondary control, and the model of assimilative and accommodative coping do not focus exclusively on how older people deal with losses; they also take the continued possibilities for growth and gains into account (Carstensen & Freund, 1994).
Successful Aging: A Matter of Disengagement or Continued Activity?
For a long time, the investigation of processes related to successful aging was dominated by two opposed conceptions: disengagement theory (Cumming & Henry, 1961) and activity theory (e.g., Lemon, Bengtson, & Peterson, 1971; Maddox, 1963, 1965, 1985).
Disengagement theory posits that the psychological energy of a person declines with age. Coinciding with a decrease in social roles in old age (e.g., because of retirement) and the anticipation of one’s death, the diminished energy was assumed to lead to a change in orientation away from activity towards preoccupation with inner aspects of oneself, life review, and one’s death (Cumming & Henry, 1961). According to disengagement theory, the most important task of old age is to disengage from involvement with society and to orient oneself towards inner aspects of the self, accepting agerelated changes and the impending death. As Cumming and Henry (1961, p. 226) put it, “the apprehension of death as a not-so-distant goal may be a time of redefinition of the self as less bound to the surrounding network of interaction. The anticipation of being apart from those nearby may accelerate withdrawal of cathexis from them, and hasten the turning of all cathexis inward—to the self for its own sake and the past for its memories.”
Disengagement theory has been criticized primarily for two reasons. First, interindividual differences in the level of activity that are apparent in middle adulthood continue to be present in old age. Disengagement can therefore not be viewed as a universal process of old age (e.g., Reichard, Livson & Peterson, 1962). Second, the loss of social roles (e.g., professional occupation) can be substituted by other activities (e.g., volunteer work) and hence does not inevitably lead to a decreased level of activity (e.g., Atchley, 1982).
In contrast to disengagement theory, activity theory posits that the maintenance of social roles and activities is crucial for successful aging. According to activity theory, the loss of social roles in old age threatens the self-definition of older people and leads to a loss of orientation and guidance for behavior in everyday life (Blau, 1981; Lemon et al., 1971; Maddox, 1963, 1965, 1985; Rosow, 1973). Hence, activity theory views the maintenance of self-defining roles through active involvement in life as one of the central processes of successful aging.
Taking a similar view, Rowe and Kahn (1998, p. 40) stressed the role of active engagement when elaborating on the difference between (merely) usual and (outstanding) successful aging: “Successful aging goes beyond potential; it involves activity, which we have labeled ‘engagement with life.’Active engagement with life takes many forms, but successful aging is most concerned with two—relationships with other people, and behavior that is productive.”
One of the more recent theories dealing with the phenomenon of reduced social contacts in old age—a phenomenon that disengagement theory claims is a sign of withdrawal from society towards life review and preparation for death, and that activity theory views as problematic for the elderly—is socioemotional selectivity theory (SST) by Carstensen and her colleagues (e.g., 1993, 1995; Carstensen, Isaacowitz, & Charles, 1999). Similar to disengagement theory, SST posits that reduced social contacts in old age are due to a limited time perspective—that is, due to the fact that older people tend to perceive their remaining time to death as relatively limited. In contrast to disengagement theory, however, SST postulates that the reduced network size does not result primarily from a deliberate withdrawal from society, but rather from the specific motivation for particular types of social relations in situations in which time perspectives are limited.
According to SST, there are two primary motivations for social interactions—emotion regulation and knowledge acquisition. Emotion regulation is best achieved with familiar and close social partners. Knowledge acquisition, on the other hand, often requires one to meet and interact with new people or with people who are emotionally not very close (namely, those who have or can give access to desired knowledge). The basic tenet of SST is that the perceived time expansion determines the relative importance of these two basic motivations for social interaction. An extended future time perspective is more strongly associated with knowledgerelated goals for social interactions. A limited time perspective, in contrast, brings about a stronger presence-orientation involving goals related to feeling states, emotional meaning, and satisfaction. Emotional meaning and satisfaction as well as emotion regulation are more easily established with familiar and close social partners than with unfamiliar or less important persons.
According to SST, the driving force behind reducing the number of social partners in old age, therefore, is a predominance of the motivation for emotion regulation over knowledge acquisition because of the older adults’ limited future time perspective. Older persons choose to be with a smaller circle of familiar social partners with whom they can have emotionally meaningful interactions. The decline in the number of social partners in old age, accordingly, does not result from withdrawing from social goals but instead reflects a stronger focus on emotion regulation.
Several empirical studies have demonstrated that the reduction of social network size in old age is primarily due to focusing on the closest social partners such as family and confidants (e.g., Field & Minkler, 1988; Lang & Carstensen, 1994; Lang, Staudinger, & Carstensen, 1998). The change in the ranking of knowledge-related and emotional goals in social relations, however, is only related to age, caused by age. When younger people are faced with time limitations and when future social opportunities are perceived as constrained, the salience of emotion goals also increases; this has been shown in studies in which younger adults were asked to imagine a limited future and older adults were asked to imagine an expansive future (e.g., Fredrickson & Carstensen, 1990), as well as in field studies with younger samples who actually experienced a very limited future time expansion, such as HIV-infected persons (Carstensen & Fredrickson, 1998) or residents of Hong Kong 2 months before the city would be handed over to the People’s Republic of China (Fung, Carstensen, & Lutz, 1999).
SST suggests that there is no universal process of continued activity or disengagement in old age, but that it is perceived time expansion that best explains whether older people prefer to focus on close, familiar social partners or are motivated to gain knowledge through knowledgeable novel social partners. This view is also consistent with the finding that activity level per se does not seem to be related to wellbeing and life satisfaction in old age. An early study by Havighurst, Neugarten, and Tobin (1968) suggests that interindividual differences in personality styles might moderate the relationship between activity and well-being. Similarly, results from the Bonn Longitudinal Study (BOLSA) show that the relationship between level of activity and well-being depends on the specific life domains or role contents under study (Thomae, 1987). Taken together, these results suggest that depending on personality, lifestyle, and life domain, high or low levels of activity can be associated with well-being in old age.
Another factor determining the relationship between activity and well-being might be how much control a person has over whether to engage in an activity. Whereas disengagement theory seems to imply that role losses are inevitable in old age, activity theory works on the assumption that older people have control over finding alternative activities in which to engage. Two important theories of successful development and aging center around the notion of control: the theory of primary and secondary control by Heckhausen and Schulz (1995) and the model of assimilative and accommodative coping by Brandtstädter and his colleagues (Brandtstädter & Greve, 1994; Brandtstädter & Renner, 1990; Brandtstädter & Wentura, 1995). Both models suggest that under conditions of reduced controllability—such as those that occur in old age because of health-related reductions in functional capacity and activity radius (Manton, 1990; Krauss Whitbourne, 1985)—disengagement from rather than persistence in the pursuit of desired activities promotes well-being. These two models are discussed in more detail later in this research paper. First, however, we present a metatheoretical framework of successful development—the model of selection, optimization, and compensation (SOC), which was first formulated by P. B. Baltes and Baltes (1980, 1990).
Selection, Optimization, and Compensation (SOC): A Metamodel of Successful Aging
The model of selection, optimization, and compensation (SOC) provides a general framework for conceptualizing processes of successful aging (P. B. Baltes & Baltes, 1990). The SOC model is based on the assumption that throughout the lifespan, individuals continually seek to successfully manage their lives through the orchestration of three processes of developmental regulation: selection, optimization, and compensation.
As a metamodel, the SOC theory (M. M. Baltes, 1987; M. M. Baltes & Carstensen, 1996, 1998; M. M. Baltes & Lang, 1997; P. B. Baltes, 1997; P. B. Baltes, & Baltes, 1990; P. B. Baltes, Dittmann-Kohli, & Dixon, 1984; Freund & Baltes, 1998, 2000; Lerner, Freund, DeStefanis, & Habermas, 2001; Marsiske et al., 1995; Wiese, Freund, & Baltes, 2000) represents a framework for the understanding of developmental continuity and change across different periods of the life span (e.g., early and late adulthood), across different levels of analysis (e.g., individual, group), and across different domains of functioning (e.g., social, cognitive, physical).
Selection, optimization, and compensation, which we define in more detail later in this section, are proposed to be universal processes of developmental regulation that can vary greatly in their phenotypic expression, depending on the sociohistorical and cultural context, the domain of functioning, and the unit of analysis at hand (P. B. Baltes, 1997). The SOC model in its general formulation therefore does not designate any specific content or mechanisms to its proposed developmental regulatory principles. In this sense, the model represents a relativistic heuristic framework. In order to understand specific manifestations of the SOC processes in particular developmental domains, it is necessary to specify the SOC processes by linking the metamodel with more specific theories pertaining to the phenomena of interest.
Taking an action-theoretical approach (e.g., Brandtstädter, 1999), one such content-driven specification of the SOC model conceptualizes expressions of selection, optimization, and compensation in the context of goal-related action (Freund & Baltes, 2000; Freund et al., 1999). This approach integrates motivational processes into a life-span perspective by considering processes of goal setting and goal pursuit within a long-term temporal perspective. In our discussion of the processes of selection, optimization, and compensation in this section, we use this action-theoretical specification of the model to illustrate specific expressions of the generalpurpose processes in the domain of personal goals.
Selection
Throughout the life span, biological, social, and individual opportunities and constraints both provide and delimit the variety of developmental pathways a person can potentially take. The number of those options, however, is usually larger than the amount of resources available to the individual. Selection—that is, focusing one’s resources on a subset of potentially available options—thus functions as a precondition for canalization and developmental specialization. One of the central functions of selection is to efficiently utilize the limited amount of available resources. In old and very old age, when resources become more constrained, selection should hence be of particular importance. Consistent with this view, Staudinger and Freund (1998) found that selecting few life domains on which to focus was particularly adaptive for older people with highly constrained resources.
In an action-theoretical framework, selection can be defined as developing, elaborating, and committing oneself to personal goals. On this level of analysis, selection directs development because personal goals guide and organize behavior across situations and time (e.g., Emmons, 1996). Successful goal selection requires developing and setting goals in domains for which resources are available or can be acquired and in domainsthat match a person’s needs and environmental demands (Freund, 1997; Heckhausen, 1999).
The SOC model distinguishes between two kinds of selection, elective selection and loss-based selection. Both aspects of selection differ in their specific developmental regulatory function. Elective selection denotes the delineation of goals in order to advance the match of a person’s needs and motives with the given or attainable resources and opportunity structures. It aims at achieving higher levels of functioning.
In contrast, loss-based selection occurs as a response to losses in previously available goal-relevant means threatening the maintenance of a goal. Loss-based selection involves changes in goals or the goal system, such as reconstructing one’s goal hierarchy by focusing on the most important goal(s), adapting standards, or substituting for goals that are no longer achievable (see also our discussion of assimilative coping, Brandtstädter & Wentura, 1995, and our discussion of compensatory secondary control, Heckhausen, 1999). The SOC model posits that loss-based selection is an important process of life mastery. Throughout the life span, individuals encounter losses in goal-relevant resources affecting their positive functioning. Loss-based selection allows focusing or redirecting resources adaptively when other means for the maintenance of positive functioning substituting the loss (compensation) are either not available or would be invested at the expense of other, more promising goals (M. M. Baltes, 1996; Heckhausen, 1999).
Selection promotes positive development in a number of ways. To hold and feel committed to goals contributes to feeling that one’s life has a purpose, thereby giving meaning to life (e.g., Klinger, 1977; Little, 1989). Furthermore, goals organize behavior into action sequences. They reduce the complexity of any given situation as they guide attention and behavior. In other words, goals can also be seen as chronically available decision rules (implemental mind-set; Gollwitzer, 1996) for directing attention and behavior to those of the numerous stimuli and behavioral options in a given situation that are goal-relevant. In this sense, goals help one to efficiently interact with one’s environment. Instead of deliberating about all of the possible alternatives one has in any given situation, people scan their environment for possibilities to pursue their goals.
Goals do not necessarily need to be conscious in order to function as guides for attention and behavior. According to the auto-motive model by Bargh and Gollwitzer (1994), the repeated activation of a goal in a certain situation leads to an association of the respective goal and situational cues. Such situational features can then automatically trigger a goal and activate goal-relevant actions. In this sense, goals that are very frequently and consistently activated can initiate and guide behavior particularly efficiently.
Optimization
Whereas selection is the first step towards positive functioning, the SOC model posits that for achieving desired outcomes in selected domains, it is crucial to acquire, apply, and refine goal-relevant means, a process that is referred to as optimization.Which means are best suited for achieving one’s goals varies according to the specific goal domain (e.g., achievement vs. social domain), personal characteristics (e.g., gender), and the sociocultural context (e.g., institutional support systems). It is possible, however, to identify a number of general processes involved in the acquisition, application, and refinement of goal-relevant means (see P. B. Baltes, 1997; Freund & Baltes, 2000; Freund et al., 1999). Later in this section, we briefly discuss some prototypical instances.
On the most general level, some sort of monitoring of the discrepancy between the actual and the desired state (goal) needs to take place (Carver & Scheier, 1995; Miller, Galanter, & Pribram, 1960). This continuous monitoring, which might occur outside of conscious awareness (Wegner, 1992), allows a constant adaptation of goal-related action. Progress toward the goal motivates the continuation of the invested goalrelevant means, whereas lack of progress or even an increase in the distance to the goal indicates that other means might be better suited for achieving the respective goal.
Another example for a general process related to optimization is the delay of immediate gratification for the sake of a more long-term payoff (e.g., Mischel, 1996). Long-term goals often require investing resources without immediate gains. Not giving in to temptations that offer short-term gratifications is thus a precondition for the persistent pursuit of a goal over an extended period of time.
One of the most important general processes of optimization is practice. As has been shown in the expertise literature, deliberate practice is a key factor for acquiring new skills and reaching peak performance (Ericsson, 1996). Repeated practice leads to the refinement of skill components, to their integration and automatization that thereby become less resource-demanding, and to free resources that can be devoted to other goal-related means. Although the role of practice might be most obvious in domains with a clear achievement aspect such as academic achievement, sports, or music (Ericsson, 1996), practice may also be important in domains with less clearly defined skills and success criteria, such as interpersonal relationships.
In old age, optimization continues to be of great importance for life management because engaging in growth-related goals generally has positive regulative functions.Anumber of studies with younger adults (e.g., Coats, Janoff-Bulman, &Alpert, 1996; Elliot & Church, 1997; Elliot & Sheldon, 1997; Elliot, Sheldon, & Church, 1997; Emmons, 1996) have shown that trying to achieve gain- or growth-oriented goals (optimization) is associated with a higher degree of self-efficacy and leads to positive emotions and well-being, whereas trying to avoid losses and functional decline is related to negative emotions and distress. In old age, when losses are prevalent and expected, it might be of particular importance for promoting well-being and a sense of self-efficacy to sustain growth- or gain-related goals and not to focus only on losses. In fact, data from the Berlin Aging Study support the positive function of optimization in old age: Older people who reported to engage in optimization also reported more positive emotions and higher satisfaction with aging (Freund & Baltes, 1998).
Compensation
How do older people manage to maintain positive functioning in the face of health-related constraints and other losses in plasticity and reserve capacity that we discussed in the first part of this research paper? One relevant strategy for the regulation of losses has already been mentioned—loss-based selection. This strategy denotes the restructuring of one’s goal system—for example, by giving up unattainable goals and developing new ones. Even in the face of losses, however, when losses are not too pervasive, goals can often be maintained by using alternative means. This process is referred to as compensation.
Compensation denotes the acquisition and use of means to counteract loss or decline in goal-related means. Typical instances are the substitution of previously available goalrelevant means by acquiring new or activating unused internal or external resources (Bäckman & Dixon, 1992; Carstensen, Hanson, & Freund, 1995; Marsiske et al., 1995). As we discussed in the context of optimization, which means are best suited for maintaining a given level of functioning in the face of loss or decline depends on the domain of functioning. Once again, such aspects of self-regulation as delay of gratification, control beliefs, and practice generally play an important role in the acquisition and investment of compensatory means. In contrast to optimization, compensation aims at counteracting or avoiding losses rather than at approaching positive states. Because of the losses associated with increasing age, aging individuals have to allocate more and more of their resources into the maintenance of functioning and the resilience against losses rather than into processes of growth (Staudinger et al., 1995). The negative effects of avoidance goals for younger age groups that were mentioned above (e.g., Coats et al., 1996; Elliot, & Church, 1997; Emmons, 1996) might be less pronounced or even absent in old age, when a focus on maintenance might be experienced as something positive (Freund & Baltes, 2000; Heckhausen, 1999). Again, data from the BerlinAging Study (Freund & Baltes, 1998) support the positive effect of compensation, showing that self-reported compensation was associated with subjective indicators of successful aging (i.e., emotional well-being, satisfaction with aging, and life satisfaction).
SOC and Age
Although selection, optimization, and compensation are conceptualized as general processes of developmental regulation that function throughout the life span, these processes also undergo developmental changes. Regarding old age, two predictions seem plausible (Freund & Baltes, 2000): On the one hand, older adults might become better at the use of SOC strategies because of their increasing life experience. On the other hand, the use of SOC strategies itself is resource dependent and effortful. As the resources available to older persons decrease, the engagement in SOC-related behaviors might become more difficult. In old age, SOC-related behaviors might therefore decline. Consistent with the latter argument, cross-sectional data revealed a decrease in self-reported SOC with increasing age (Freund & Baltes, 1998, 2000). Despite such a decline in self-reported SOC behaviors, however, selection, optimization, and compensation continued to have positive associations to well-being (Freund & Baltes, 1998, 1999, 2000) and to everyday functioning (M. M. Baltes & Lang, 1997) well into old age.
In sum, the SOC model conceptualizes successful aging as the interplay of three processes:
- Developing, elaborating, and committing to those goals of functioning that promote a fit between personal needs or preferences, environmental, societal, or biological demands and actual or acquirable resources (selection). In old age, when an individual is confronted with changes in personal needs or preferences, demands, and resources, selection of goals in which all three of these factors converge should be of particular importance for positive functioning.
- Acquiring, refining, and investing (internal or external) resources into the pursuit of the selected goals (optimization). To promote gains and growth in old age—a life phase in which developmental losses outweigh developmental gains—it is important to acquire new or activate previously unused goal-relevant external or internal means (e.g., social support).
- Acquiring and investing resources into selected domains of functioning in order to counteract losses of previously available goal-relevant means (compensation). Given the inevitable losses of old age, an important facet of successful aging is the management of losses and the maintenance of functioning. Because compensatory efforts also require resources, careful selection of goals on which to focus in the face of loss (i.e., loss-based selection) is essential for successful aging.
In the following discussion, we present two models of successful aging that are compatible with the SOC metamodel but that put a particular emphasis on the controllability of events: the model of primary and secondary control by Heckhausen and Schulz (1995) and the model of assimilative and accommodative coping by Brandtstädter and colleagues (e.g., Brandtstädter & Renner, 1990).
The Model of Optimization in Primary and Secondary Control (OPS)
Converging with the SOC model, the model of optimization in primary and secondary control (OPS model) by Heckhausen and Schulz stresses the importance of selectivity and compensation for developmental regulation and successful aging (Heckhausen, 1999; Heckhausen & Schulz, 1995, 1999; Schulz, 1986; Schulz & Heckhausen, 1996). Unlike the developers of the SOC model, Heckhausen and Schulz (1998, pp. 55–56) “conceptualize optimization as a higher order regulatory process” that balances and maintains selectivity and compensation. In the OPS model, selectivity denotes the focused investment of resources into selected goals, whereas compensation refers to strategies helping to attain a selected goal when internal resources are insufficient or when faced with failure or losses.
Heckhausen and Schulz propose that the challenges of life can be mastered by jointly employing two modes of control: primary and secondary control. According to their model, humans have an innate need to control their world. The primary way to achieve control is by employing instrumental efforts to modify the environment according to one’s goals (i.e., primary control). If such control strategies directed at the external world are not available or if they fail, an internal focus on changing one’s goals and standards or engaging in self-protective attributions or social comparisons takes over (i.e., secondary control). The main function of secondary control is to focus and protect motivational resources for primary control. In general, Heckhausen and Schulz propose that the maximization of primary control potential is the criterion of adaptive functioning across the life span. This is particularly difficult in old age, when losses become more prominent and less controllable, thereby depleting the potential for primary control (Schulz, 1986). Thus, in old age, secondary control strategies should gain more and more in importance for successful developmental regulation.
Heckhausen and Schulz distinguish two forms of primary and secondary control strategies—namely selective and compensatory forms. Selective primary control denotes actions that are directly aimed at goal achievement, such as investing time, effort, and skills into the pursuit of goals. Compensatory primary control—that is, the investment of external resources (e.g., help of others) or the acquisition of alternative resources takes place when available internal resources are not sufficient for achieving one’s goals. This process is particularly important in old age when internal resources are subject to decline and losses. Selective secondary control refers to enhanced selectivity of resource investment into already existing goals through motivational processes such as enhancing commitment to a given goal. Finally, compensatory secondary control buffers negative effects of failure in primary control strivings through cognitive reframing of goals, such as decreasing the desirability of unobtainable goals or favorable social comparisons. These strategies—again of particular importance in old age when resource-intensive goals might become increasingly difficult to achieve due to loss and decline in relevant resources—should contribute to the longterm primary control potential because they work against the negative motivational effects of failure experience and contribute to the maintenance of self-efficacy and well-being.
According to Heckhausen and Schulz, none of these four types of control strategies alone is sufficient to bring about successful development. Instead, the four types of control have to be orchestrated according to the opportunity structure and constraints of an individual’s developmental ecology. For instance, Wrosch and Heckhausen (1999) showed that control strategies differ systematically between younger and older adults who encounter the same situation—namely, separation or divorce from a long-term partner. Based on demographic data, they assumed that these two age groups differ in their opportunities for finding a new partner, such that younger adults have much better chances than do older adults. In accordance with propositions of the OPS model, younger separated adults reported more primary control strivings for attaining partnership goals, whereas older separated adults reported higher levels of goal deactivation (compensatory secondary control). Moreover, Wrosch and Heckhausen could show that goal disengagement was positively related to change in positive affect over time in older adults but negatively related in younger adults.
With regard to aging, Heckhausen, Schulz, and Wrosch (1998) found that in general, endorsement of control strategies increases from young to old adulthood. The one exception to this age pattern pertained to compensatory secondary control, which was reported least in all age groups. The authors interpreted this finding as supporting their notion of the primacy of primary control. Moreover, they concluded that “overall, with increasing age adults appear to know about, appreciate, and maybe rely more on strategies of developmental regulation” (Heckhausen & Schulz, 1998, p. 70).All four types of control strategies were shown to be positively related to self-esteem, which further supports the importance of primary and secondary control strategies for successful aging.
The Model of Assimilative and Accommodative Coping
Brandtstädter and his colleagues (Brandtstädter & Greve, 1994; Brandtstädter & Renner, 1990; Brandtstädter & Wentura, 1995; Brandtstädter, Wentura, & Rothermund, 1999) proposed a model that addresses the question what processes can explain the so-called paradox of stability in well-being despite the many losses and constraints older persons encounter. According to their model, people use primarily two distinct, complementary forms of coping to achieve “a match between actual developmental outcomes or prospects and personal goals and ambitions” (Brandtstädter et al., 1999, pp. 375–376)—namely, assimilation and accommodation. Assimilation refers to tenacious goal pursuit by modifying the environment or the circumstances so that they fit personal goals. It involves actional (i.e., intentional) neutralization of a mismatch between the current and the desired states. In contrast, accommodation denotes processes of flexible goal adjustment by changing, downgrading, or discarding personal goals or lowering one’s level of aspirations so that they fit the circumstances. It is characterized by mental neutralizations of a mismatch between the actual and the desired state that work primarily on a nonintentional, unconscious level.
Brandtstädter and colleagues (e.g., Brandtstädter et al., 1999) posit that people first use assimilative strategies to cope with loss—that is, they first try to overcome obstacles blocking their goals by actional neutralizations. If goals remain blocked despite assimilative attempts, a gradual shift to the accommodative mode occurs. The gradual shift from the assimilative to the accommodative mode is theorized to occur in the following order:When attempts at altering the situation do not succeed, auxiliary activities will be activated or acquired. When these auxiliary attempts do not lead to the desired outcomes, external aids or support systems might be engaged (cf. the concept of proxy control by Bandura, 1982). When all of these instrumental actions do not help to alter the situation in the desired way, people, according to Brandtstädter, feel helpless and depressed. This state, however, is only temporary and marks the shift to accommodative processes such as disengagement from goals or adjustment of standards take place.
Brandtstädter et al. (1999), however, also point out that the shift from assimilative to accommodative coping does not always follow this fixed temporal pattern; rather, it depends on personal and situational factors. Brandtstädter and Wentura (1995) list three key factors affecting assimilative and accommodative tendencies in opposite directions: (a) importance of the goal—when a goal is of great personal importance, assimilative tendencies are activated, whereas accommodative tendencies are inhibited; (b) probability of success—if there is a sufficient probability of success in achieving a goal, assimilative coping prevails over accommodative coping; and (c) accessibility of palliative information—contextual or chronically available palliative information (e.g., social norms, personal attitudes) that eases the acceptance of a previously aversive situation fosters a shift to the accommodative mode.
Brandtstädter and colleagues predict a general shift during aging from assimilative to accommodative coping. When losses begin to occur, people should first respond with assimilative coping directed at actively counteracting losses. When with increasing age, losses begin to become more widespread and hence both the probability of success and the resources to engage in assimilative actions decline, accommodative coping should gain in importance. This theoretically expected pattern, which has been empirically confirmed (Brandtstädter & Renner, 1990; Brandtstädter, Rothermund, & Schmitz, 1997), is seen as important for successful aging because Brandtstädter et al. (1999, p. 391) “consider the process of continuously readjusting goals and pBibliography: to action reserves as crucial to the maintenance of self-esteem and even efficacy in later life.” Again, empirical evidence supports this hypothesis. Brandtstädter and Renner (1990) could show that accommodative tendencies such as flexible goal adjustment buffer the negative association between perceived developmental deficits and life satisfaction as well as buffer the negative effect of health-related problems on subjective well-being (Brandtstädter, Wentura, & Greve, 1993).
According to this model, successful aging can be characterized primarily as a coping process that shifts from actively counteracting beginning age-related losses to cognitively restructuring personal goals or standards: “A comprehensive theoretical view [of successful aging] . . . must also account for the fact that to maintain a sense of efficacy and selfesteem, personal goals and self-evaluative standards have to be continually revised and adjusted to the changes that characterize the processes of physical, psychological, and social aging” (Brandtstädter et al., 1999, p. 382).
Summary
Old age is a relatively new phenomenon because life expectancy has only relatively recently extended into old age. In many modern countries, this increase in life expectancy has been co-occurring with a decline in fertility rates. This has drastically altered the population’s composition. Declining proportions of working-age people have to ensure adequate living conditions for a growing number of old people. To meet this challenge, gerontology needs to provide knowledge about positive or successful aging and the conditions that foster it. In this research paper, we reviewed current knowledge and theory on this topic.
In the first part of the paper, we elaborated the specific context of old age in four life domains: physiological changes, cognitive functioning, social relations, and everyday competence. From this discussion, we inferred (a) that with advancing age, the ratio of developmental gains and losses becomes increasingly negative; (b) that old age, like any other phase in life, is characterized by tremendous intraand interindividual heterogeneity; and (c) that it is necessary to distinguish between young-old and old-old age. Many individuals in their 60s and 70s exhibit relatively high levels of functioning, whereas in very old age (85 years and older) the detrimental effects of aging become more pronounced.
Given the unfavorable ratio of developmental gains to losses in older adulthood, the term successful aging sounds like an oxymoron. This lead us to the question of how to best define successful aging. We discussed the current state of research on this question in the second part of this research paper. On an abstract level, researchers typically agree that successful aging can be defined as the simultaneous maximization of gains and minimization of losses. What exactly constitute gains and losses, however, must be specified depending on the specific research question at hand. Presumably because of the inherent value-judgement required for delineating criteria for successful aging, no generally accepted set of criteria characterizing successful aging exists. It is, however, generally acknowledged that an encompassing characterization of how well a person is aging should comprise objective as well as subjective, short-term as well as long-term, general as well as domain-specific, and static as well as dynamic indicators.
In the third part of this research paper, we shifted the focus away from discussing criterion-centered approaches to defining successful aging to reviewing theories that address the question of processes underlying successful aging. Recently, the role of proactive processes in aging has been increasingly recognized. A basic assumption underlying this notion is that development is a dynamic process of both reacting to and proactively shaping one’s environment as well as oneself (e.g., Lawton, 1989; Lerner & Busch-Rossnagel, 1981). According to this view, individuals continuously adapt to their changing environment, act upon their environment, and actively create environments that fit their needs (e.g., move to a ground-floor apartment in which a wheelchair can be used when mobility is impaired).
Recent models of successful aging stress the role of motivational processes in understanding developmental regulation in old age, such as the model of selection, optimization, and compensation (P. B. Baltes, 1997; P. B. Baltes & Baltes, 1990; Freund et al., 1999; Marsiske et al., 1995), the model of assimilative and accommodative coping (e.g., Brandtstädter & Greve, 1994; Brandtstädter & Renner, 1990), and the model of primary and secondary control (e.g., Heckhausen & Schulz, 1995).According to these models, an important way in which individuals play an active role in their development is by choosing, committing to, and pursuing personal goals. By adapting goals and standards to the increasingly constrained resources (e.g., health-related decline), older people can maintain their well-being and a certain degree of control.
At this point, most of the research on processes of developmental regulation in old age is primarily concerned with understanding how and under what conditions these processes contribute to successful aging. We hope, however, that identifying the central processes of successful aging will help to develop prevention or intervention programs to enhance the quality of older persons’lives in the not-so-distant future.
Bibliography:
- Aiken, L. R. (1989). Later life (3rd ed.). Hillsdale, NJ: Erlbaum.
- Anstey, K. J., Lord, S. R., & Williams, P. (1997). Strength in the lower limbs, visual contrast, and simple reaction time predict cognition in older women. Psychology and Aging, 12, 137–144.
- Antonucci, T. C. (1985). Personal characteristics, social support, and social behavior. In R. H. Binstock & E. Shanas (Eds.), Handbook of aging and the social sciences (2nd ed., pp. 94– 128). New York: Van Nostrand Reinhold.
- Antonucci, T. C. (1990). Social supports and social relationships. In R. H. Binstock & L. K. George (Eds.), Handbook of aging and the social sciences (3rd ed., pp. 205–226). San Diego, CA: Academic Press.
- Antonucci,T. C. (1991).Attachment, social support, and coping with negative life events in mature adulthood. In E. M. Cummings, A. L. Greene, & K. H. Karraker (Eds.), Life-span developmental psychology: Perspectives on stress and coping (pp. 261–276). Hillsdale, NJ: Erlbaum.
- Antonucci, T. C., & Akiyama, H. (1994). Convoys of attachment and social relations in children, adolescents, and adults. In F. Nestmann & K. Hurrelmann (Eds.), Social networks and social support in childhood and adolescence (pp. 37–52). Berlin: de Gruyter.
- Antonucci, T. C., & Akiyama, H. (1995). Convoys of social relations: Family and friendship within a lifespan context. In Blieszner & V. H. Bedford (Eds.), Handbook of aging and the family (pp. 355–371). Westport, CT: Greenwood Press.
- Antonucci, T. C., & Jackson, J. S. (1987). Social support, interpersonal efficacy, and health: A life course perspective. In L. L. Carstensen & B. A. Edelstein (Eds.), Handbook of clinical gerontology (pp. 291–311). New York: Pergamon Press.
- Atchley, R. C. (1982). The aging self. Psychotherapy: Theory, Research and Practice, 19, 388–396.
- Bäckman, L., & Dixon, R. A. (1992). Psychological compensation: A theoretical framework. Psychological Bulletin, 112, 1–25.
- Baltes, M. M. (1987). Erfolgreiches Altern als Ausdruck von Verhaltenskompetenz und Umweltqualität [Successful aging as expression of behavioral competence and environmental quality]. In C. Niemitz (Ed.), Der Mensch im Zusammenspiel von AnlageundUmwelt[Thehumanbeingintheinteractionofnature and nuture] (pp. 353–376). Frankfurt, Germany: Suhrkamp.
- Baltes, M. M. (1996). The many faces of dependency in old age. New York: Cambridge University Press.
- Baltes, M. M., & Carstensen, L. L. (1996). The process of successful ageing. Ageing and Society, 16, 397–422.
- Baltes, M. M., & Carstensen, L. L. (1998). Social psychological theories and their applications to aging: From individual to collective. In V. L. Bengtson & K. W. Schaie (Eds.), Handbook of theories of aging (pp. 209–226). New York: Springer.
- Baltes, M. M., & Lang, F. R. (1997). Everyday functioning and successful aging: The impact of resources. Psychology and Aging, 12, 433–443.
- Baltes, M. M., Maas, I., Wilms, H.-U., Borchelt, M., & Little, T. D. (1999). Everyday competence in old and very old age: Theoretical considerations and empirical findings. In P. B. Baltes & K. U. Mayer (Eds.), The Berlin Aging Study. Aging from 70 to 100 (pp. 384–402). New York: Cambridge University Press.
- Baltes, M. M., Mayr, U., Borchelt, M., Maas, I., & Wilms, H.-U. (1993). Everyday competence in old and very old age: An interdisciplinary perspective. Ageing and Society, 13, 657–680.
- Baltes, M. M., Wahl, H.-W., & Reichert, M. (1991). Successful aging in long-term care institutions? In K. W. Schaie & M. P. Lawton (Eds.), Annual review of gerontology and geriatrics (Vol. 11, pp. 311–337). New York: Springer.
- Baltes, M. M., & Wilms, H.-U. (1995). Alltagskompetenz im Alter [Everyday competence in old age]. In R. Oerter & L. Montada (Eds.), Entwicklungspsychologie [Developmental psychology] (pp.1127–1136).Weinheim,Germany:PsychologieVerlagsUnion.
- Baltes, P. B. (1987). Theoretical propositions of life-span developmental psychology: On the dynamics between growth and decline. Developmental Psychology, 23, 611–626.
- Baltes, P. B. (1989). The dynamics between growth and decline. Contemporary Psychology, 34, 983–984.
- Baltes, P. B. (1997). On the incomplete architecture of human ontogeny: Selection, optimization, and compensation as foundation of developmental theory. American Psychologist, 52, 366–380.
- Baltes, P. B., & Baltes, M. M. (1980). Plasticity and variability in psychological aging: Methodological and theoretical issues. In G. Gurski (Ed.), Determining the effects of aging on the central nervous system (pp. 41–60). Berlin: Schering.
- Baltes, P. B., & Baltes, M. M. (1990). Psychological perspectives on successful aging: The model of selective optimization with compensation. In P. B. Baltes & M. M. Baltes (Eds.), Successful aging: Perspectives from the behavioral sciences (pp. 1–34). New York: Cambridge University Press.
- Baltes, P. B., Dittmann-Kohli, F., & Dixon, R. A. (1984). New perspectives on the development of intelligence in adulthood: Toward a dual-process conception. In P. B. Baltes & J. O. G. Brim (Eds.), Life-span development and behavior (Vol. 6, pp. 33–76). New York: Academic Press.
- Baltes, P. B., Dittmann-Kohli, F., & Kliegl, R. (1986). Reserve capacity of the elderly in aging-sensitive tests of fluid intelligence: Replication and extension. Psychology and Aging, 1, 172–177.
- Baltes, P. B., & Kliegl, R. (1992). Further testing of limits of cognitive plasticity: Negative age differences in a mnemonic skill are robust. Developmental Psychology, 28, 121–125.
- Baltes, P. B., & Lindenberger, U. (1988). On the range of cognitive plasticity in old age as a function of experience: 15 years of intervention research. Behavior Therapy, 19, 283–300.
- Baltes, P. B., Lindenberger, U., & Staudinger, U. M. (1998). Life-span theory in developmental psychology. In R. M. Lerner (Ed.), Handbook of child psychology: Vol. 1. Theoretical models of human development (5th ed., pp. 1029–1143). New York: Wiley.
- Baltes, P. B., Sowarka, D., & Kliegl, R. (1989). Cognitive training research on fluid intelligence in old age: What can older adults achieve by themselves? Psychology and Aging, 4, 217–221.
- Baltes, P. B., Staudinger, U. M., & Lindenberger, U. (1999). Lifespan psychology: Theory and application to intellectual functioning. Annual Review of Psychology, 50, 471–507.
- Baltes, P. B., Staudinger, U. M., Maercker, U. M., & Smith, J. (1995). People nominated as wise: A comparative study of wisdomrelated knowledge. Psychology and Aging, 10, 155–166.
- Baltes, P. B., & Willis, S. L. (1982). Enhancement (plasticity) of intellectual functioning in old age: Penn State’s Adult Development and Enrichment Project (ADEPT). In F. I. M. Craik & S. Trehub (Eds.), Aging and cognitive processes (pp. 353–389). New York: Plenum Press.
- Bandura, A. (1982). Self-efficacy mechanism in human agency. American Psychologist, 37, 122–147.
- Bargh, J. A., & Gollwitzer, P. M. (1994). Environmental control of goal-directed action: Automatic and strategic contingencies between situations and behavior. In W. D. Spaulding (Ed.), Nebraska Symposium on Motivation: Vol. 41. Integrative views of motivation, cognition, and emotion (pp. 71–124). Lincoln: University of Nebraska Press.
- Bauco, C., Golosio, F., Cinti, A. M., Borriello, C., Raganato, P., Cicconetti, P., Cacciafesta, M., & Marigliano, V. (1996). Functional status and well-being of centenarians. Archives of Gerontology and Geriatry, 5, 363–366.
- Bebbington, A. C. (1988). The expectation of life without disability in England and Wales. Social Science Medicine, 27, 321–326.
- Berg, C. A., & Klaszynski, P. A. (1996). Practical intelligence and problem solving: Searching for perspectives. In F. BlanchardFields & T. M. Hess (Eds.), Perspectives on cognitive change in adulthood and aging (pp. 323–357). New York: McGraw-Hill.
- Blau, Z. S. (1981). Aging in a changing society (2nd ed.). New York: Franklin Watts.
- Bortz, W. M. (1982). Disuse and aging. Journal of the American Medical Association, 248, 1203–1208.
- Bosman, E. A. (1993). Age-related differences in the motoric aspects of transcription typing skill. Psychology and Aging, 8, 87–102.
- Bosman, E. A., & Charness, N. (1996). Age-related differences in skilled performance and skill acquisition. In F. BlanchardFields & T. M. Hess (Eds.), Perspectives on cognitive change in adulthood and aging (pp. 428–453). New York: McGraw-Hill.
- Boult, C., Kane, R. L., Louis, T. A., Boult, L., & McCaffrey, D. (1994). Chronic conditions that lead to functional limitations in the elderly. Journal of Gerontology: Medical Sciences, 49, M28–M36.
- Bowling, A. (1994). Social networks and social support among older people and implications for emotional well-being and psychiatric morbidity. International Review of Psychiatry, 6, 41–58.
- Bradburn, N. M. (1969). The structure of psychological wellbeing. Chicago: Aldine.
- Bradsher, J. E. (1997). Older women and widowhood. In J. M. Coyle (Ed.), Handbook on women and aging (pp. 418–429). Westport, CT: Greenwood Press.
- Brandtstädter, J. (1998). Action perspectives on human development. In R. M. Lerner (Ed.), Handbook of child psychology: Vol. 1. Theoretical models of human development (5th ed., pp. 807–866). New York: Wiley.
- Brandtstädter, J. (1999). The self in action and development: Cultural, biosocial, and ontogenetic bases of intentional selfdevelopment. In J. Brandtstädter & R. M. Lerner (Eds.), Action and self-development: Theory and research through the life span (pp. 37–65). Thousand Oaks, CA: Sage.
- Brandtstädter, J., & Greve, W. (1994). The aging self: Stabilizing and protective processes. Developmental Review, 14, 52–80.
- Brandtstädter, J., & Renner, G. (1990). Tenacious goal pursuit and flexible goal adjustment: Explication and age-related analysis of assimilative and accommodative strategies of coping. Psychology and Aging, 5, 58–67.
- Brandtstädter, J., Rothermund, K., & Schmitz, U. (1997). Coping resources in later life. European Review of Applied Psychology, 47, 107–114.
- Brandtstädter, J., & Wentura, D. (1995). Adjustment to shifting possibility frontiers in later life: Complementary adaptive modes. In R. A. Dixon & L. Bäckman (Eds.), Compensating for psychological deficits and declines: Managing losses and promoting gains (pp. 83–106). Hillsdale, NJ: Erlbaum.
- Brandtstädter, J., Wentura, D., & Greve, W. (1993). Adaptive resources of the aging self: Outlines of an emergent perspective. Journal of Behavioral Development, 16, 323–349.
- Brandtstädter, J.,Wentura, D., & Rothermund, K. (1999). Intentional self-development through adulthood and later life: Tenacious pursuit and flexible adjustment of goals. In J. Brandtstädter & R. M. Lerner (Eds.), Action and self-development: Theory and research through the life span (pp. 373–400). Thousand Oaks, CA: Sage.
- Brickman, P., Coates, D., & Janoff-Bulman, R. (1978). Lottery winners and accident victims: Is happiness relative? Journal of Personality and Social Psychology, 37, 917–927.
- Brubaker, T. H. (1990). Families in later life: A burgeoning research area. Journal of Marriage and the Family, 52, 959–981.
- Campbell, A., Converse, P. E., & Rodgers, W. L. (1976). The quality of American life: Perceptions, evaluations, and satisfaction. New York: Russell Sage Foundation.
- Carstensen, L. L. (1993). Motivation for social contact across the life-span: A theory of socioemotional selectivity. In J. E. Jacobs et al. (Ed.), Nebraska Symposium on Motivation, 1992: Developmental perspectives on motivation. Current theory and research in motivation (Vol. 40, pp. 209–254). Lincoln: University of Nebraska Press.
- Carstensen, L. L. (1995). Evidence for a life-span theory of socioemotional selectivity. Current Directions in Psychological Science, 4, 151–156.
- Carstensen, L. L., & Fredrickson, B. F. (1998). Socioemotional selectivity in healthy older people and younger people living with the human inmmunodeficiency virus: The centrality of emotion when the future is constrained. Health Psychology, 17, 1–10.
- Carstensen, L. L., & Freund, A. M. (1994). The resilience of the self. Developmental Review, 14, 81–92.
- Carstensen, L. L., Hanson, K. A., & Freund, A. M. (1995). Selection and compensation in adulthood. In R. A. Dixon & L. Bäckman (Eds.), Compensating for psychological deficits and declines: Managing losses and promoting gains (pp. 107–126). Mahwah, NJ: Erlbaum.
- Carstensen, L. L., Isaacowitz, D. M., & Charles, S. T. (1999). Taking time seriously: A theory of socioemotional selectivity. American Psychologist, 54, 165–181.
- Carver, C. S., & Scheier, M. F. (1995). On the self-regulation of behavior. Cambridge, UK: Cambridge University Press.
- Case, R. (1985). Intellectual development: From birth to adulthood. New York: Academic Press.
- Cattell, R. B. (1971). Abilities: Their structure, growth, and action. Boston: Houghton Mifflin.
- Charness, N. (1981a). Search in chess: Age and skill differences. Journal of Experimental Psychology: Human Perception and Performance, 7, 467–476.
- Charness, N. (1981b). Visual short-term memory and aging in chess players. Journals of Gerontology, 36, 615–619.
- Charness, N. (1983). Age, skill, and bridge bidding: A chronometric analysis. Journal of Verbal Learning and Verbal Behavior, 22, 406–416.
- Charness, N. (1987). Component processes in bridge bidding and novel problem solving tasks. Canadian Journal of Psychology, 41, 223–243.
- Cicirelli, V. G. (1982). Sibling influence throughout the life span. In M. E. Lamb & B. Sutton-Smith (Eds.), Sibling relationships: Their nature and significance across the lifespan (pp. 267–284). Hillsdale, NJ: Erlbaum.
- Cicirelli, V. G. (1985). The role of siblings as family caregivers. In W. J. Sauer & R. T. Coward (Eds.), Social support networks and the care of the elderly (pp. 93–107). New York: Springer.
- Clayton, V. P., & Birren, J. E. (1980). The development of wisdom across the life span: A reexamination of an ancient topic. In P. B. Baltes & J. O. G. Brim (Eds.), Life-span development and behavior (Vol. 3, pp. 103–135). New York: Academic Press.
- Coats, E. J., Janoff-Bulman, R., & Alpert, N. (1996). Approach versus avoidance goals: Differences in self-evaluation and well-being. Personality and Social Psychology Bulletin, 22, 1057–1067.
- Connidis, I. A. (1989). Siblings as friends in later life. American Behavioral Scientist, 33, 81–93.
- Cooper, B. (1997). Epidemiology of the dementias in late life. In R. Jacoby & C. Oppenheimer (Eds.), Psychiatry in the elderly (pp. 439–453). Oxford, UK: Oxford University Press.
- Crimmins, E. M., Hayward, M. D., & Saito, Y. (1996). Differentials in active life expectancy in the older population of the United States. Journals of Gerontology: Social Sciences, 51B, S111– S120.
- Cumming, E., & Henry, W. E. (1961). Growing old. New York: Basic Books.
- Diehl, M. (1998). Everyday competence in later life: Current status and future directions. Gerontologist, 38(4), 422–433.
- Diener, E. (1999, November). Measurement and findings on subjective well-being. Distinguished Lecture presented at the Max Planck Institute for Human Development, Berlin, Germany.
- Diener, E., Suh, E. K., Lucas, R. E., & Smith, H. L. (1999). Subjective well-being: Three decades of progress. Psychological Bulletin, 125, 276–302.
- Dinkel, R. H. (1994). Demographische Alterung: Ein Überblick unter besonderer Berücksichtigung der Mortalitätsentwicklung [Demographic aging: An overview with special consideration of the development of mortality]. In P. B. Baltes, J. Mittelstraß, & U. M. Staudinger (Eds.), Alter und Altern: Ein interdisziplinärer Studientext zur Gerontologie [Age and Aging: An interdisciplinary textbook on gerontology] (pp. 62–93). Berlin: de Gruyter.
- Dykstra, P. A. (1993). The differential availability of relationships and the provision and effectiveness of support to older adults. Journal of Social and Personal Relationships, 10, 355–370.
- Elliot, A. J., & Church, M. A. (1997). A hierarchical model of approach and avoidance motivation. Journal of Personality and Social Psychology, 72, 218–232.
- Elliot, A. J., & Sheldon, K. M. (1997). Avoidance achievement motivation: A personal goal analysis. Journal of Personality and Social Psychology, 73, 171–185.
- Elliot, A. J., Sheldon, K. M., & Church, M. A. (1997). Avoidance personal goals and subjective well-being. Personality and Social Psychology Bulletin, 23, 915–927.
- Emmons, R. A. (1996). Striving and feeling: Personal goals and subjective well-being. In P. M. Gollwitzer & J. A. Bargh (Eds.), The psychology of action: Linking cognition and motivation to behavior (pp. 313–337). New York: Guilford Press.
- Ericsson, K. A. (1996). The road to excellence: The acquisition of expert performance in the arts and sciences, sports and games. Mahwah, NJ: Erlbaum.
- Feldman, J. J., Makuc, D. M., Kleinman, J. C., & Huntley, J. C. (1989). National trends in educational differences in mortality. American Journal of Epidemiology, 129, 919–933.
- Ferring, D., & Filipp, S.-H. (1995). The structure of subjective wellbeing in the elderly: Atest of different models by structural equation modeling. European Journal of Psychological Assessment, 11,
- Field, D. (1999). Continuity and change in friendships in advanced old age: Findings from the Berkeley Older Generations Study. International Journal of Aging and Human Development, 48, 325–346.
- Field, D., & Minkler, M. (1988). Continuity and change in social support between young-old and old-old or very-old age. Journal of Gerontology: Psychological Sciences, 43, P100–P106.
- Frederick, S., & Loewenstein, G. (1999). Hedonic adaptation. In D. Kahneman, E. Diener, & N. Schwarz (Eds.), Well-being: The foundations of hedonic psychology (pp. 302–329). New York: Russell Sage Foundation.
- Fredrickson, B. C., & Carstensen, L. L. (1990). Choosing social partners: How old age and anticipated endings make people more selective. Psychology and Aging, 5, 163–171.
- Freund, A. M. (1997). Individuating age-salience: A psychological perspective on the salience of age in the life course. Human Development, 40, 287–292.
- Freund, A. M., & Baltes, P. B. (1998). Selection, optimization, and compensation as strategies of life-management: Correlations with subjective indicators of successful aging. Psychology and Aging, 13, 531–543.
- Freund, A. M., & Baltes, P. B. (1999). Selection, optimization, and compensation as strategies of life management: Correction to Freund and Baltes (1998). Psychology and Aging, 14, 700–702.
- Freund, A. M., & Baltes, P. B. (2000). The orchestration of selection, optimization, and compensation: An action-theoretical conceptualization of a theory of developmental regulation. In W. J. Perrig & A. Grob (Eds.), Control of human behavior, mental processes and consciousness (pp. 35–58). Mahwah, NJ: Erlbaum.
- Freund, A. M., Li, K. Z. H., & Baltes, P. B. (1999). Successful development and aging: The role of selection, optimization, and compensation. In J. Brandtstädter & R. M. Lerner (Eds.), Action and self-development: Theory and research through the life span (pp. 401–434). Thousand Oaks, CA: Sage.
- Fries, J. F. (1990). Medical perspectives upon successful aging. In P. B. Baltes & M. M. Baltes (Eds.), Successful aging: Perspectives from the behavioral sciences (pp. 35–49). Cambridge, UK: Cambridge University Press.
- Fung, H., Carstensen, L. L., & Lutz, A. (1999). Influence of time on social pBibliography:: Implications for life-span development. Psychology and Aging, 14, 595–604.
- Furner, S. E., Rudberg, M. A., & Cassel, C. K. (1995). Medical conditions differentially affect the development of IADLdisability: Implications for medical care and research. Gerontologist, 35, 444–450.
- Gallagher-Thompson, D., Futterman, A., Farberow, N., Thompson, L. W., & Peterson, J. (1993). The impact of spousal bereavement on older widows and widowers. In M. S. Stroebe, W. Stroebe, & R. O. Hansson (Eds.), Handbook of bereavement: Theory, research, and intervention (pp. 227–239). Cambridge, UK: Cambridge University Press.
- George, L. K. (1981). Subjective well-being: Conceptual and methodological issues. In C. Eisdorfer (Ed.), Annual review of gerontology and geriatrics (Vol. 2). New York: Springer.
- Goetting, A. (1986). The developmental tasks of siblingship over the life cycle. Journal of Marriage and the Family, 48, 703–714.
- Gollwitzer, P. M. (1996). Das Rubikonmodell der Handlungsphasen [The rubicon model of action phases]. In J. Kuhl & H. Heckhausen (Eds.), Motivation, Volition, und Handlung [Motivation, volition, action] (Vol. 4, pp. 531–582). Göttingen, Germany: Hogrefe.
- Havighurst, R. J. (1963). Successful aging. In R. H. Williams, C. Tibbitts, & W. Donahue (Eds.), The process of aging: Social and psychological perspectives (Vol. 1, pp. 299–320). New York: Atherton Press.
- Havighurst, R. J., & Albrecht, R. (1953). Older people. New York: Longmans Green.
- Havighurst, R. J., Neugarten, B. L., & Tobin, S. S. (1968). Disengagement and patterns of aging. Gerontologist, 4,
- Hayslip, B. (1989). Alternative mechanisms for improvements in fluid ability performance among older adults. Psychology and Aging, 4, 122–124.
- Heckhausen, J. (1999). Developmental regulation in adulthood: Age-normative and sociostructural constraints as adaptive challenges. New York: Cambridge University Press.
- Heckhausen, J., Dixon, R. A., & Baltes, P. B. (1989). Gains and losses in development throughout adulthood as perceived by different adult age groups. Developmental Psychology, 25, 109–121.
- Heckhausen, J., & Schulz, R. (1995). A life-span theory of control. Psychological Review, 102, 284–304.
- Heckhausen, J., & Schulz, R. (1998). Developmental regulation in adulthood: Selection and compensation via primary and secondary control. In J. Heckhausen & C. S. Dweck (Eds.), Motivation and self-regulation across the life span (pp. 50–77). New York: Cambridge University Press.
- Heckhausen, J., & Schulz, R. (1999). Biological and societal canalizations and individuals’ developmental goals. In J. Brandtstädter & R. Lerner (Eds.), Action and self-development: Theory and research through the life span (pp. 67–103). London, UK: Sage.
- Heckhausen, J., Schulz, R., & Wrosch, C. (1998). Developmental regulation in adulthood: Optimization in primary and secondary control. Berlin: Max Planck Institute for Human Development.
- Heller, K., & Mansbach, W. E. (1984). The multifaceted nature of social support in a community sample of elderly women. Journal of Social Issues, 40, 99–113.
- Hess, T. M., & Pullen, S. M. (1996). Memory in context. In F. Blanchard-Fields & T. M. Hess (Eds.), Perspectives on cognitive change in adulthood and aging (pp. 387–427). New York: McGraw-Hill.
- Hobfoll, S. E. (2001). The influence of culture, community, and the nested-self in the stress process: Advancing conservation of resources theory. Applied Psychology: An International Review, 50, 337–421.
- Hofman, A., Rocca, W., Brayne, C., Breteler, M. B. B., Clarke, M., Cooper, B., Copeland, J. R., Dartigues, J. F., da Silva Droux, A., & Hagnell, O. (1991). The prevalence of dementia in Europe: A collaborative study of 1980–1990 findings. International Journal of Epidemiology, 20, 736–748.
- Horgas, A. L., Wilms, H.-U., & Baltes, M. M. (1998). Daily life in very old age: Everyday activities as expression of successful living. Gerontologist, 38, 556–568.
- Horn, J. L. (1982). The theory of fluid and crystallized intelligence in relation to concepts of cognitive psychology and aging in adulthood. In F. I. M. Craik & S. Trehub (Eds.), Aging and cognitive processes (pp. 237–278). New York: Plenum Press.
- Jagger, C., Clarke, M., & Clarke, S. J. (1991). Getting older— feeling younger: The changing health profile of the elderly. International Journal of Epidemiology, 20, 234–238.
- Jorm, A. F., Korten, A. E., & Henderson, A. S. (1987). The prevalence of dementia: A quantitative integration of the literature. Acta Psychiatrica Scandinavica, 76, 465–479.
- Kahana,E.,&Kahana,B.(1996).Conceptualandempiricaladvances in understanding aging well through proactive adaptation. InV. L. Bengtson (Ed.), Adulthood and aging: Research on continuities and discontinuities (pp. 18–40). NewYork: Springer.
- Kahn,R.L.,&Antonucci,T.C.(1980).Convoysoverthelifecourse. Attachment, roles, and social support. In P. B. Baltes & O. G.
- Brim (Eds.), Life-span development and behavior (pp. 254– 283). New York:Academic Press.
- Kail, R. (1991). Developmental change in speed of processing during childhood and adolescence. Psychological Bulletin, 109, 490–501.
- Kail, R., & Salthouse, T. A. (1994). Processing speed as a mental capacity. Acta Psychologica, 86, 199–225.
- Kannisto, V., Turpeinen, O., & Nieminen, M. (1999). Finnish life tables since 1751. Rostock, Germany: Max Planck Institute for Demographic Research. Retrieved from www.demographicresearch.org/Volumes/Vol1/1 (August 2000).
- Katz, S., Ford, A. B., Moskowitz, R. W., Jackson, B. A., & Jaffe, M. W. (1963). Studies of illness in the aged. The index of ADL: A standardized measure of biological and psychosocial function. Journal of the American Medical Association, 185, 914–919.
- Kessler, R. C., & McLeod, J. D. (1985). Social support and mental health in community samples. In S. Cohen & S. L. Syme (Eds.), Social support and health (pp. 219–240). New York: Academic Press.
- Kliegl, R., Smith, J., & Baltes, P. B. (1990). On the locus and process of magnification of age differences during mnemonic training. Developmental Psychology, 26, 894–904.
- Klinger, E. (1977). Meaning and void: Inner experience and the incentives in people’s lives. Minneapolis: University of Minnesota Press.
- Knopf, M., Kolodziej, P., & Preussler, W. (1990). Der ältere Mensch als Experte: Literaturübersicht über die Rolle von Expertenwissen für die kognitive Leistungsfähigkeit im höheren Alter [The elderly person as expert: Literature review on the role of expert knowledge for cognitive performance in older age]. Zeitschrift für Gerontopsychologie und -psychiatrie, 4, 233–248.
- Labouvie-Vief, G., Chiodo, L. M., Goguen, L. A., Diehl, M., & Orwoll, L. (1995). Representations of self across the life span. Psychology and Aging, 10, 404–415.
- Lang, F. R., & Carstensen, L. L. (1994). Close emotional relationships in late life: Further support for proactive aging in the social domain. Psychology and Aging, 2, 315–324.
- Lang, F. R., & Carstensen, L. L. (1998). Social relationships and adaptation in later life. In A. S. Bellack & M. Hersen (Ed.), Comprehensive clinical psychology: Vol. 7. Clinical geropsychology (pp. 55–72). Oxford, UK: Elsevier Science.
- Lang, F. R., Staudinger, U. M., & Carstensen, L. L. (1998). Perspectives on socioemotional selectivity in late life: How personality and social context do (and do not) make a difference. Journal of Gerontology: Psychological Sciences, 53B, 21–30.
- Lawton, M. P. (1983). Environment and other determinants of wellbeing in older people. Gerontologist, 23, 349–357.
- Lawton, M. P. (1985). The elderly in context: Perspectives from environmental psychology and gerontology. Environment and Behavior, 17, 501–519.
- Lawton, M. P. (1989). Environmental proactivity in older people. In V. L. Bengston & K. W. Schaie (Eds.), The course of later life: Research and reflections (pp. 15–23). New York: Springer.
- Lawton, M. P., & Brody, E. M. (1969). Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist, 9, 179–186.
- Lawton, M. P., Kleban, M. H., & Dean, J. (1993). Affect and age: Cross-sectional comparisons of structure and prevalence. Psychology and Aging, 8, 165–175.
- Lawton, M. P., & Nahemow, L. (1973). Ecology and the aging process. In C. Eisdorfer & M. P. Lawton (Eds.), The psychology of adult development and aging (pp. 619–674). Washington, DC: American Psychological Association.
- Lemon, B. W., Bengtson, V. L., & Peterson, J. A. (1971). An exploration of the activity theory of aging: Activity types and life satisfactions among in-movers to a retirement community. Journal of Gerontology, 27, 511–523.
- Lerner, R. M. (Ed.). (1998). The handbook of child psychology: Theoretical models of human development (5th ed., Vol. 1). New York: Wiley.
- Lerner, R. M., & Busch-Rossnagel, N. A. (1981). Individuals as producers of their development: Conceptual and empirical bases. In R. M. Lerner & N. A. Busch-Rossnagel (Eds.), Individuals as producers of their development: A life-span perspective (pp. 1–36). New York: Academic Press.
- Lerner, R. M., Freund, A. M., DeStefanis, I., & Habermas, T. (2001). Understanding Developmental Regulation in Adolescence: The use of the selection, optimization, and compensation model. Human Development, 44(1), 29–50.
- Levenson, R. W., Carstensen, L. L., Friesen, W. V., & Ekman, P. (1991). The influence of age and gender on affect, physiology, and their interrelations: A study of long-term marriages. Journal of Personality and Social Psychology, 67, 56–68.
- Li, S.-C., & Lindenberger, U. (1999). Cross-level unification: A computational exploration of the link between deterioration of neurotransmitter systems and dedifferentiation of cognitive abilities in old age. In L. G. Nilsson & H. Markowitsch (Eds.), Cognitive neuroscience of memory (pp. 104–146). Toronto, Canada: Hogrefe & Huber.
- Lindenberger, U., & Reischies, F. M. (1999). Limits and potentials of intellectual functioning in old age. In P. B. Baltes & K. U. Mayer (Eds.), The Berlin Aging Study: Aging from 70 to 100 (Vol. 12, pp. 329–359). New York: Cambridge University Press.
- Little, B. R. (1989). Personal projects analysis: Trivial pursuits, magnificent obsessions, and the search for coherence. New York: Springer.
- Lund, D. A., Caserta, M. S., & Dimond, M. F. (1993). The course of spousal bereavement in later life. In M. S. Stroebe, W. Stroebe, & R. O. Hansson (Eds.), Handbook of bereavement: Theory, research, and intervention (pp. 240–254). Cambridge, UK: Cambridge University Press.
- Maddox, G. L. (1963). Activity and morale: A longitudinal study of selected elderly subjects. Social Forces, 42, 195–204.
- Maddox, G. L. (1965). Fact and artefact: Evidence bearing on disengagement theory. Human Development, 8, 117–130.
- Maddox, G. L. (1985). The process of disengagement: Unfalsifiable theories never die [Special Issue]. Gerontologist, 25,
- Maddox, G. L., & Clark, D. O. (1992). Trajectories of functional impairment in later life. Journal of Health and Social Behavior, 33, 114–125.
- Magnusson, D. (Ed.). (1996). The life-span development of individuals: Behavioural, neurobiological and psychosocial perspectives. Cambridge, UK: Cambridge University Press.
- Manton, K. G. (1990). Mortality and morbidity. In R. Binstock & L. George (Eds.), Handbook of aging and social sciences (3rd ed., pp. 64–89). San Diego, CA: Academic Press.
- Manton, K. G., Corder, L. S., & Stallard, E. (1993). Estimates of change in chronic disability and institutional incidence and prevalence rates in the U.S. elderly population from the 1982, 1984, and 1989 National Long Term Care Survey. Journal of Gerontology: Social Sciences, 48, S153–S166.
- Mares, M.-L. (1995). The aging family. In M. A. Fitzpatrick & A. L. Vangelisti (Eds.), Explaining family interactions (pp. 344–374). Thousand Oaks, CA: Sage.
- Marsiske, M., Lang, F. R., Baltes, P. B., & Baltes, M. M. (1995). Selective optimization with compensation: Life-span perspectives on successful human development. In R. A. Dixon & L. Bäckman (Eds.), Compensating for psychological deficits and declines: Managing losses and promoting gains (pp. 35–79). Mahwah, NJ: Erlbaum.
- Matthews, K. A., Kelsey, S. F., Meilahn, E. N., Kuller, L. H., & Wing, R. R. (1989). Educational attainment and behavioral and biological risk factors for coronary heart disease in middle-aged women. American Journal of Epidemiology, 129, 1132–1144.
- Medina, J. J. (1996). The clock of ages. Why we age—how we age— winding back the clock. Cambridge, UK: Cambridge University Press.
- Meeks, C. B., Nickols, S. Y., & Sweaney, A. L. (1999). Demographic comparisons of aging in five selected countries. Journal of Family and Economic Issues, 20, 223–250.
- Miller, G. A., Galanter, E., & Pribram, K.-H. (1960). Plans of structure of behavior. New York: Holt, Rinehart, and Winston.
- Mischel, W. (1996). From good intentions to willpower. In P. M. Gollwitzer & J. A. Bargh (Eds.), The psychology of action (pp. 197–218). New York: Guilford Press.
- Palmore, E. (1981). Social patterns in normal aging: Findings from the Duke Longitudinal Study. Durham, NC: Duke University Press.
- Palmore, E. B., & Kivett, V. R. (1985). Change in life satisfaction. In E. B. Balmore, E. W. Busse, G. L. Maddox, J. B. Nowline, & I. C. Siegler (Eds.), Normal aging: Vol. 3. Reports from the Duke Longitudinal Studies, 1975–1984 (pp. 373–380). Durham, NC: Duke University Press.
- Peterson, C. (2000). The future of optimism. American Psychologist, 55, 44–55.
- Pulkkinen, L. (2000). Developmental psychology. In K. Pawlik & M.R.Rosenzweig(Eds.),International handbookof psychology: Vol. 2. Adulthood and aging (pp. 261–282). Thousand Oaks, CA: Sage.
- Reichard, S., Livson, F., & Peterson, P. G. (1962). Aging and personality. A study of eighty-seven older men. New York: Arno Press.
- Riley, M. W. (1998). Letters to the editor. Gerontologist, 38,
- Rosow, I. (1973). The social context of the aging self. Gerontologist, 13, 82–87.
- Ross, H. G., & Milgram, J. I. (1982). Important variables in adult sibling relationships: A qualitative analysis. In M. E. Lamb & B. Sutton-Smith (Eds.), Sibling relationships: Their nature and significance across the lifespan (pp. 225–266). Hillsdale, NJ: Erlbaum.
- Rowe, J. W., & Kahn, R. L. (1987). Human aging: Usual and successful. Science, 237, 143–149.
- Rowe, J. W., & Kahn, R. L. (1998). Successful aging. New York: Pantheon Books.
- Ryff, C. D. (1989). Happiness is everything, or is it? Explorations on the meaning of psychological well-being. Journal of Personality and Social Psychology, 57, 1069–1081.
- Ryff, C. D. (1995). Psychological well-being in adult life. Current Directions in Psychological Science, 4, 99–104.
- Salthouse, T. A. (1984). Effects of age and skill in typing. Journal of Experimental Psychology: General, 113, 345–371.
- Salthouse, T. A., Hancock, H. E., Meinz, E. J., & Hambrick, D. Z. (1996). Interrelations of age, visual acuity, and cognitive functioning. Journal of Gerontology: Psychological Sciences, 51B, P317–P330.
- Salthouse, T. A., & Saults, J. S. (1987). Multiple spans in transcription typing. Journal of Applied Psychology, 72, 187–196.
- Schaie, K. W. (1994). The course of adult intellectual development. American Psychologist, 49, 304–313.
- Schaie, K. W. (1996). Intellectual development in adulthood: The Seattle Longitudinal Study. New York: Cambridge University Press.
- Schaie, K. W., & Willis, S. L. (1986). Can intellectual decline in the elderly be reversed? Developmental Psychology, 22, 223–232.
- Schaie, K. W., & Willis, S. L. (1999). Theories of everyday competence and aging. In V. L. Bengtson & K. W. Schaie (Eds.), Handbook of theories of aging (pp. 174–195). New York: Springer.
- Schulz, R. (1986). Successful aging: Balancing primary and secondary control. Adult Development and Aging News, 13, 2–4.
- Schulz, R., & Heckhausen, J. (1996). A life-span model of successful aging. American Psychologist, 51, 702–714.
- Schwarz, N., & Strack, F. (1999). Reports of subjective well-being: Judgmental processes and their methodological implications. In Kahneman, E. Diener, & N. Schwarz (Eds.), Well-being: The foundations of hedonic psychology (pp. 61–84). New York: Russell Sage Foundation.
- Schwarzer, R., & Leppin, A. (1991). Social support and health: A theoretical and empirical overview. Journal of Social and Personal Relationships, 8, 99–127.
- Scott, J. P. (1983). Siblings and other kin. In T. H. Brubaker (Ed.), Family relationships in later life (pp. 47–62). Beverly Hills, CA: Sage.
- Seeman, T. E. (1996). Social ties and health: The benefits of social integration. Annals of Epidemiology, 6, 442–451.
- Seligman, M. E. P. (1991). Learned optimism. New York: Knopf.
- Siegler, I. C., & Costa, P. T., Jr. (1985). Health behavior relationships. In J. E. Birren & K. W. Schaie (Eds.), Handbook of the psychology of aging (2nd ed., pp. 144–166). New York: Van Nostrand Reinhold.
- Singer, T. (2000). Testing-the-Limits in einer mnemonischen Fähigkeit: Eine Studie zur kognitiven Plastizität im hohen Alter [Testing-the-Limits in a mnemonic technique: A study of cognitive plasticity in very old age]. Berlin, Germany: Free University. Retrieved 2001, from www.Diss.FU-Berlin.de/2000/ 78/index. html
- Smith, J., Fleeson, W., Geiselmann, B., Settersten, R. A., Jr., & Kunzmann, U. (1999). Well-being in very old age: Predictions from objective life conditions and subjective experience. In P. B. Baltes & K. U. Mayer (Eds.), The Berlin Aging Study: Aging from 70 to 100 (pp. 450–471). New York: Cambridge University Press.
- Smith, J., & Goodnow J. J. (1999). Unasked-for support and unsolicited advice: Age and the quality of social experience. Psychology and Aging, 14, 108– 121.
- Staudinger, U. M. (1996). Wisdom and the social-interactive foundation of the mind. In P. B. Baltes & U. M. Staudinger (Eds.), Interactive minds: Life-span perspectives on the social foundation of cognition (pp. 276–318). New York: Cambridge University Press.
- Staudinger, U. M., & Freund, A. M. (1998). Krank und “arm” im hohen Alter und trotzdem guten Mutes? Untersuchungen im Rahmen eines Modells psychologischer Widerstandsfähigkeit [Sick and “poor” in old age and still in good spirits? A study of psychological resilience]. Zeitschrift für Klinische Psychologie, 27, 78–85.
- Staudinger, U. M., Marsiske, M., & Baltes, P.B. (1995). Resilience and reserve capacity in later adulthood: Potentials and limits of development across the life span. In D. Cicchetti & D. J. Cohen (Eds.), Developmental psychopathology: Vol. 2. Risk, disorder, and adaptation (pp. 801–847). New York: Wiley.
- Steinhagen-Thiessen, E., & Borchelt, M. (1999). Morbidity, medication, and functional limitations in very old age. In P. B. Baltes & K. U. Mayer (Eds.), The Berlin Aging Study: Aging from 70 to 100 (pp. 131–166). New York: Cambridge University Press.
- Steinhagen-Thiessen, E., Gerok, W., & Borchelt, M. (1994). Innere Medizin und Geriatrie [Internal medicine and geriatrics]. In P. B. Baltes, J. Mittelstraß, & U. M. Staudinger (Eds.), Alter und Altern: Ein interdisziplinärer Studientext zur Gerontologie [Age and aging: An interdisciplinary textbook on gerontology] (pp. 124–150). Berlin: de Gruyter.
- Sternberg, R. J. (1990). Wisdom and its relations to intelligence and creativity. In R. J. Sternberg (Ed.), Wisdom: Its nature, origins, and development (pp. 142–149). New York: Cambridge University Press.
- Stroebe, M. S., & Stroebe, W. (1993). The mortality of bereavement: A review. In M. S. Stroebe, W. Stroebe, & R. O. Hansson (Eds.), Handbook of bereavement: Theory, research, and intervention (pp. 175–226). Cambridge, UK: Cambridge University Press.
- Thomae, H. E. (1976). Patterns of aging. Basel, Switzerland: Karger.
- Thomae, H. E. (1987). Alternsformen: Wege zu ihrer methodischen und begrifflichen Erfassung [Forms of aging: Approaches for their methodological and conceptual assessment]. In U. Lehr & H. Thomae (Eds.), Formen seelischen Alterns [Forms of mental aging] (pp. 173–195). Stuttgart, Germany: Enke.
- Tsai, J. L., Levenson, R. W., & Carstensen, L. L. (2000). Autonomic, subjective, and expressive responses to emotional films in older and younger Chinese Americans and European Americans. Psychology and Aging, 15, 684–693.
- Tucker, J. S., Schwartz, J. E., Clark, K. M., & Friedman, H. S. (1999).Age-related changes in the associations of social network ties with mortality risk. Psychology and Aging, 14, 564–571.
- United Nations. (1996). The ageing of the world’s population. Retrieved August 2000, from http://www.un.org/ecosocdev/ geninfo/ageing/ageing-e.htm
- van Sonderen, E., Ormel, J., Brilman, E., & van Linden van den Heuvell, C.-M. (1990). Personal network delineation: Acomparison of the exchange, affective and role-relation approach. In K. C. P. M. Knipscheer & T. C. Antonucci (Eds.), Social network research (pp. 101–120). Amsterdam: Swets & Zeitlinger.
- Vaupel, J. (1995). Life expectancy. In G. L. Maddox (Ed.), The encyclopedia of aging (pp. 559–560). New York: Springer.
- Vaupel, J. W., Carey, J. R., Christensen, K., Johnson, T. E., Yashin, A. I., Holm, N. V., Iachine, I. A., Kannisto, V., Khazaeli, A. A., Liedo, P., Longo, V. D., Zeng, Y., Manton, K. G., & Curtsinger, J. W. (1998). Biodemographic trajectories of longevity. Science, 280, 855–860.
- Verbrugge, L. M. (1989). The twain meet: Empirical explanation of sex differences in health and mortality. Journal of Health and Social Behavior, 30, 282–304.
- Verhaegen, P., Marcoen, A., & Goossens, L. (1992). Improving memory performance in the aged through mnemonic training: A metaanalytic study. Psychology and Aging, 7, 242–251.
- Wagner, M., Schütze, Y., & Lang, F. R. (1999). Social relationships in old age. In P. B. Baltes & K. U. Mayer (Eds.), The Berlin Aging Study: Aging from 70 to 100 (pp. 282–301). New York: Cambridge University Press.
- Wegner, D. M. (1992). You can’t always think what you want: Problems in the suppression of unwanted thoughts. In M. Zanna (Ed.), Advances in experimental social psychology (Vol. 25, pp. 193–225). San Diego, CA: Academic Press.
- Whitbourne, S. K. (1985). The aging body. New York: Springer.
- Wiese, B. S., Freund, A. M., & Baltes, P. B. (2000). Selection, optimization, and compensation: An action-related approach to work and partnership. Journal of Vocational Behavior, 57, 273– 300.
- Willis, S. L. (1996). Everyday problem solving. In J. E. Birren & K. W. Schaie (Eds.), Handbook of the psychology of aging (4th ed., pp. 287–307). San Diego, CA: Academic Press.
- World Health Organization. (1998). Fact Sheet Nr 135. Population aging: A public health challenge. Retrieved August 2000, from http://www.who.int/inf-fs/fact135.html
- Wrosch, C., & Heckhausen, J. (1999). Control processes before and after passing a developmental deadline: Activation and deactivation of intimate relationship goals. Journal of Personality and Social Psychology, 77, 415–427.
- Zarit, S. H., & Eggebeen, D. J. (1995). Parent-child relationships in adulthood and old age. In M. H. Bornstein (Ed.), Handbook of parenting: Vol. 1. Children and parenting (pp. 119–140). Mahwah, NJ: Erlbaum.
ORDER HIGH QUALITY CUSTOM PAPER

Always on-time

Plagiarism-Free

100% Confidentiality