
Sample Operant Conditioning And Clinical Psychology Research Paper. Browse other research paper examples and check the list of research paper topics for more inspiration. If you need a religion research paper written according to all the academic standards, you can always turn to our experienced writers for help. This is how your paper can get an A! Feel free to contact our research paper writing service for professional assistance. We offer high-quality assignments for reasonable rates.
The application of operant conditioning to issues confronting clinical psychology has a strong foundation in the basic science of B. F. Skinner. The use of operant principles in clinical psychology focuses on altering the environment to increase useful behaviors or decrease clinically maladaptive behaviors. Modern operant theory continues to extend the original model and the scope of the clinical problems it can address, and new therapies continue to be developed.
Academic Writing, Editing, Proofreading, And Problem Solving Services
Get 10% OFF with 24START discount code
1. The Basic Operant Model
Operant theory was preceded by the law of effect as proposed by Edward L. Thorndike. Early versions of the law of effect stated that behaviors that produce satisfying effects tend to increase in frequency while behaviors that produce discomfort tend to become less frequent. B. F. Skinner recognized that attending only to behavior missed an important point. A behavior can produce a good effect in one situation but a very different effect in a different circumstance. In part, an appreciation of the importance of the function of behavior in the specific context in which it occurred led to the identification of the principles of operant conditioning.
An operant gains its name from the fact that the behavior in question operates on the environment or produces a certain consequence. An operant is defined by the consequence it produces and not by the physical appearance or form (also called topography) of the behavior. Operant (also called instrumental) conditioning is typically presented in what is called the ‘multi-term contingency.’ The analysis of a behavior takes place in the context of the circumstances in which it occurs. A common representation of the operant using three explanatory terms is presented in Fig. 1. The conventional symbols are indicated in bold above the name and descriptions.
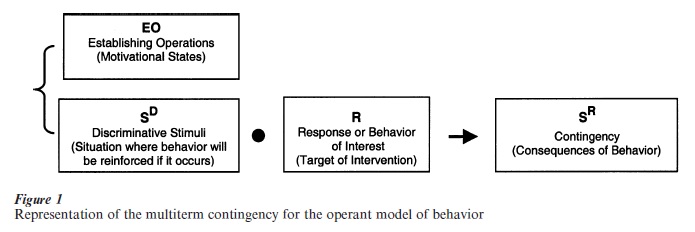
Reading from left to right the diagram can be understood to indicate that under certain conditions a behavior will occur and, depending on what follows the behavior, the behavior will be more or less likely to occur in the future under the same circumstances. Looking in more detail at the diagram, the environmental influences that set the occasion for a behavior to occur are shown in the brackets on the left and should be considered together. The discriminative stimulus (SD) is a stimulus in the presence of which the probability of a particular contingent consequence for a behavior or class of behaviors is greater than when it is not present. Bracketed with the discriminative stimulus is the establishing operation (EO). Establishing operations are any environmental changes that momentarily alter the effectiveness of a discriminative stimulus to evoke the behavior of interest and affect the rate of that response.
The ‘R’ indicates the response of interest. Responses can be overt actions or private events such as thoughts, feelings, and emotions so long as there are some observable correlates of the private events (Skinner 1945). Some critics of operant conditioning incorrectly state that only overt behavior and not private events can be studied and treated using an operant approach. In fact, operant conditioning assumes thoughts and feelings are better understood as responses to be addressed in treatment rather than causes of other behaviors (Hayes and Brownstein 1986).
The ‘SR’ term indicates the contingency that follows the behavior and influences the probability of the preceding behavior occurring again under the same or similar conditions. The notation of ‘SR’ is used, because typically the contingency is a stimulus that acts as a reinforcer. The term ‘reinforcer’ has a specific meaning in operant conditioning. A reinforcer is a stimulus that increases the probability of a given response in a particular situation when it is presented following that response and contingent upon it. The arrow indicates the temporal flow of the response being followed by the contingency. The other notation in the diagram is the dot between the discriminative stimuli and the response. The dot is interpreted as a probability function. That is, given the presence of a discriminative stimulus, there is a probability that the response will be emitted given the organism’s history.
1.1 Acquisition Of Behavior
Consider this simple example to clarify these terms. In the absence of intimate friendships and following social-skills training in therapy (EO), a client meets a prospective friend (SD) and makes a social overture to them (R) that leads to the formation of a new friendship (SR, in this case a reinforcer for approaching people as prospective friends). This sequence of behaviors leads to the strengthening of the response of initiating social contact.
Behavior is strengthened when it is followed by a reinforcing consequence. Generally, the more frequently the behavior of interest is followed by a reinforcer, the more quickly the behavior will become established. There are other well-researched factors that affect the rate of acquisition and stability of behavior (Ferster and Skinner 1957).
Distinctions are made for various types of contingencies. The most fundamental distinction is be- tween reinforcement and punishment. Any contingent stimulus that leads to an increase in the preceding behavior is called a reinforcer. Any contingency that leads to a decrease in the preceding behavior is called a punisher. The terminology is further refined by identifying whether the contingent stimulus is applied or removed to establish its effect. When a contingent stimulus is applied, it is termed positive; when a contingent stimulus is removed, it is termed negative. Table 1 clarifies the terminology of contingent stimuli.
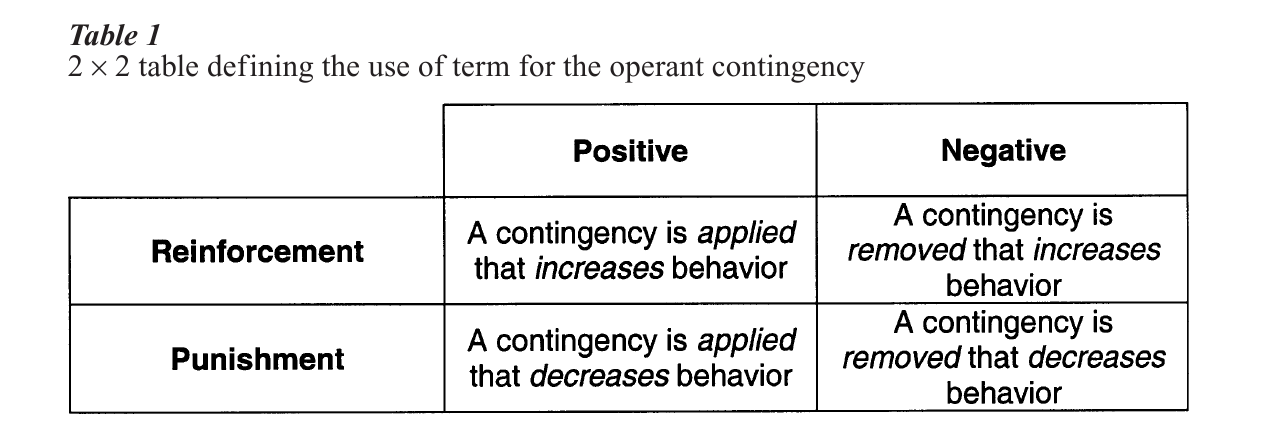
Whether a contingency is determined to be reinforcement or punishment is determined by the effect it has on the preceding behavior, not the intention of the supplier of the contingency. For example, even if a parent intends to punish a child’s tantrum by scolding them in order to decrease rate, if the scolding actually increases the tantrums (due to parental attention, perhaps) then the scolding has functioned as positive reinforcement, regardless of the intention of the parent. Thus, it is important to understand that exactly what type of contingency is operating is wholly determined by the observed function of the contingency on the response of interest.
A common misunderstanding about contingencies is that the modifiers ‘positive’ and ‘negative’ imply some moral good or bad property of the contingency. This is not the case. The terms ‘positive’ and ‘negative’ refer only to whether the contingency (i.e., the re- inforcement or punishment) is applied (positive) or removed (negative). A positive reinforcer refers to a contingency that, when applied, increases the rate of responding. A negative punisher refers to the removal of contingency that produces a reduction in the rate of responding.
1.2 Generalization
When an operant behavior has been reinforced in the presence of a particular SD, the same behavior may still be emitted in the presence of similar but not identical stimulus conditions. When an operant is emitted in the presence of a stimulus similar to the original SD, this is referred to as stimulus generalization. For example, if one learns to answer the door when a doorbell of a particular sound rings, one will likely answer a door when a doorbell of a somewhat different ring occurs, even if one has never heard that particular doorbell sound before. This is an example of stimulus generalization. Strictly speaking, generalization occurs when some actual physical property of the original SD is shared with another stimulus in the presence of which a response is emitted and reinforced. A doorbell’s sound may be similarly pitched and thus the operant (opening the door) may be emitted, even though the behavior has never been reinforced in the presence of that exact tone before. However, for the phenomenon to be considered generalization, there must be some formal property of the stimuli that are common. In the doorbell example, the formal property was some quality of the sound.
1.3 Extinction
Behavior that is established by operant conditioning can undergo extinction when the behavior that occurs in the presence of the SD is no longer followed by the SR. One of the characteristics of extinction of operant behavior is that when the SR is removed, the organism may increase the frequency of the behavior initially and often change the topography of the behavior slightly. This is called an extinction burst and can lead to the expression of new behavior that may lead to reinforcement. If reinforcement is not forthcoming, the behavior will decrease to its pre-reinforcement baseline (referred to as the free operant level).
2. Early Applications Of Operant Conditioning
There have been many applications of operant conditioning in the clinical literature. One example, in particular, demonstrates an important philosophical perspective taken by clinical operant therapists. Under the assumption that behavior is the product of environmental contingencies, two researchers, Teodoro Ayllon and Nathan Azrin (1968), studied chronically hospitalized patients at a state hospital. The patients had been in the hospital for many years and many had been diagnosed with schizophrenia and other severe forms of psychopathology. The researchers provided no direct treatment to the patients but instead altered the behavior of the staff. They assumed that the staff were inadvertently reinforcing maladaptive behavior and failing to attend to positive patient behaviors properly. Their sole intervention was to have the staff reinforce adaptive behaviors when the patients emitted them, by giving them tokens that were redeemable for a variety of reinforcers, and ignore maladaptive behaviors. This intervention is referred to as a token economy. Remarkable improvements resulted, including a number of instances where patients who had been institutionalized for many years prior to the introduction of the token economy were functioning well enough to be discharged.
Another notable early application of operant principles to clinical problems addressed severe problems in children. O. Ivar Lovaas (1977) was among early autism researchers who used operant principles to stop self-destructive behavior and establish language. One characteristic of autistic behavior is impaired or absent language. Lovaas used reinforcement principles to establish the utterance of sounds by reinforcing sounds and then withholding the reinforcement and waiting for an extinction burst to produce sounds more like the target sound. When closer approximations to target sounds occurred, they were quickly reinforced. This use of operant conditioning to build increasingly more complex behavior is called shaping by successive approximation. While the process of teaching language in this population was slow, it can be very successful. Further work at shaping verbal and social skills has produced profound improvement in verbal and social behavior in a population that had been difficult to treat previously (Lovaas 1987).
3. Clinical Interventions For Each Term Of The Operant Model
An operant analysis of clinical problems requires that behavior be understood as an act in context. What this means is that in order to understand a behavior, one has to understand its function in the context in which it occurs. As a simple clinical example, crying could function to express sadness, to get support, to terminate an aversive conversation, to express overwhelming happiness, or to get attention. To understand the act of crying, one would have to understand the conditions in which it occurs and the consequences that follow the crying contingently. To say that someone is crying does not demonstrate an adequate understanding of the controlling variables. If a clinician were to treat someone’s crying as a reflection of sadness or depression, when its function was actually to terminate a conversation that was not going the client’s way, the therapist would not achieve a good clinical outcome. When a clinician tries to understand a clinical problem, they perform a functional analysis, or an analysis of the stimulus functions of each term in the operant model (Kanfer and Saslow 1969).
It is useful to think of how problems and interventions may occur for each term of the operant model. Table 2 describes each term shown in the model followed by a description of the functional problem, a description of the process by which the problem might emerge, a clinical example, and the type of possible intervention that might be used to address the clinical problem.
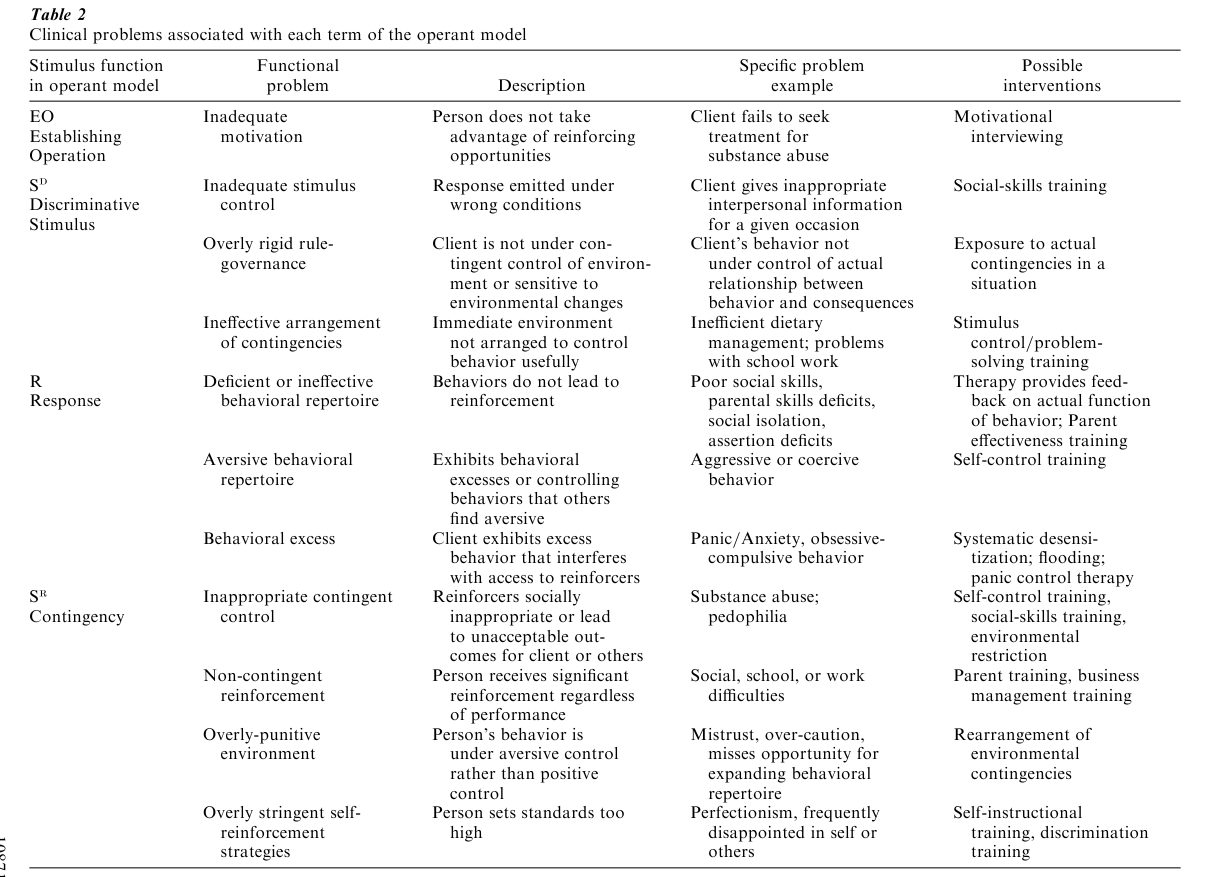
One can see that in many cases, treatment involves techniques that provide training to better discriminate conditions that indicate when a response will lead to a particular desirable or undesirable outcome. An assessment of the adequacy or frequency of a particular response is also often useful. Many times an intervention focuses on shaping a better functional response for a particular set of stimulus conditions. This may take the form of social-skills training, modeling, or training by successive approximations. There are many clinical situations when clients are taught how to better apply contingencies that affect the behavior of people around them. For example, parent effectiveness training focuses on the proper and effective application contingency management to increase useful behavior in children. The same principles can be used to increase appropriate student behavior in school or increase productivity in a business environment.
Influencing establishing operations or motivational variables is the clinical intervention with the least well-developed clinical technology. In laboratory research, deprivational states are frequently used to establish the function of a discriminative stimulus for a response that will be reinforced by food. In clinical practice, inducing deprivational states is often not practical or ethical. While parents might deprive a child of their dinner, behavior therapists do not have access to such operations. Recently, motivational interview techniques have been developed to emphasize the importance of therapy and increase its reinforcing properties. These techniques have been applied with some positive effect in the area of addictions treatment (Miller et al. 1992), but the strength of the effect and the exact mechanism of action are not clear.
4. Clinical Interventions Involving Operant And Respondent Conditioning
Respondent (also known as classical, or Pavlovian) conditioning involves the pairing of unconditioned and conditioned stimuli, which ultimately leads to a conditioned stimulus that elicits a conditioned response. One of the more useful clinical heuristics has been research on how respondent and operant conditioning can combine to explain important clinical problems.
The best-known problem that has been addressed by considering both operant and respondent conditioning is the theory of the acquisition and maintenance of phobic behaviors. It has been suggested that phobic behaviors are acquired by classical conditioning but maintained by operant conditioning. Consider the simple example of someone bitten by a dog. In respondent conditioning terms, the dog bite is an unconditioned stimulus that produces the unconditioned response of pain and fear. Following such an incident, the next time the person approaches a dog, their fear and anxiety rises as the stimulus (the dog) gets closer. So far, the acquisition of the fearful response can be understood using a classical conditioning paradigm. If the person were to approach a variety of dogs, the fearful response would extinguish naturally, because extinction in classical conditioning is accomplished by presenting the conditioned stimulus (a dog) in the absence of the unconditioned stimulus (the dog bite). If this were the case, phobic responses would extinguish naturally over time. However, in many instances when one sees the dog and anxiety increases, a person simply turns around and walks away, thus avoiding the feared object. When that happens, the avoidance behavior is negatively reinforced (increased) by the removal of the anxiety. This increases the probability of avoiding the dog the next time such a stimulus is encountered. The avoidance of the phobic object prevents the natural extinction of phobic anxiety, because the phobic object (now a conditioned stimulus) is avoided and therefore extinction cannot occur.
Avoidance is an important issue in clinical psychology. Avoidance responses are operants that prevent the occurrence of aversive consequences before they are actually experienced. This behavior is maintained by negative reinforcement. Clinically, the liability of avoidance behavior is that the person engaging in such behavior does not experience the opportunity to test whether the anticipated aversive consequences are still in effect. Thus, the circumstances that led to the initial aversive consequences may have changed, but if the person continues to avoid the original stimulus conditions, the changes will go undetected. There may also be avoidance of other stimuli due to generalization that leads to additional restrictions in healthy functioning.
Several clinical interventions address such problems. Treatments for phobias involve therapeutic interventions that prevent or remove the instrumental benefits of avoidance. Phobia treatment involves a classical conditioning paradigm in which the behavior therapist uses exposure to the conditioned stimulus to bring about extinction. The key to successful treatment is the prevention of avoidance, which would negatively reinforce the phobic behavior (Barlow 1990).
Another clinical problem that is treated, in part, by preventing avoidance behavior is obsessive-compulsive disorder (OCD). In OCD, the client experiences intrusive thoughts or images that produce anxiety. For example, someone might be obsessed with a concern that they have failed to lock their house adequately. The thoughts are high in frequency, do not feel natural to the client, and are not under the voluntary control of the client. Obsessions are thoughts or images. They are often accompanied by compulsive behaviors that serve to reduce the obsessive thoughts. In this example, a client may go back repeatedly to check that the front door is locked, preventing them from going to work. The psychological intervention used to treat OCD is exposure to the situation that produces the obsessive behavior and response prevention so that the compulsive behaviors are not emitted (Foa et al. 1980). Eventually, the anxiety associated with the problematic stimulus extinguishes, because the function of acting to reduce the distress extinguishes.
5. Future Directions In Operant Conditioning Research And Treatment
In the last 15 years there have been significant advances in operant theory. Perhaps the most important advances address the limitations of the application of the operant conceptualization of stimulus generalization to verbal behavior. Humans are unique in their ability to engage in certain kinds of verbal behavior. Earlier, stimulus generalization was defined as when a stimulus with similar physical or formal properties to the original discriminative stimulus is also followed by a response that is subsequently reinforced. However, in the instance of verbal behavior, there are stimuli that have no formal properties in common that can still serve equivalent functions. A simple instance is when the written word ‘g-r-e-e-n,’ the sound of the word ‘green’ when pronounced, and the color green all serve the same stimulus function without necessarily ever having appeared together. There are no physical similarities shared by these stimuli. They can be trained to substitute for each other so that any one stimulus can entail the functions of each of the others. When each stimulus can entail the functions of all the others and demonstrate certain experimental properties (reflexivity, symmetry, transitivity), they are said to form an equivalence class.
The clinical implication for humans is that stimuli can take on the functions of other stimuli without ever having been directly learned. Though the process is debated (Barnes-Holmes et al. in press, Sidman 1986, 1994), it is clear that one can construct functionally equivalent relationships between stimuli in complex ways. What this means clinically is that a client can respond to a variety of stimuli as if they all had the same direct learning history, even if they did not. While there are experimental methods for training these relationships, they often emerge without a person knowing that an equivalent relationship is functioning or how it came to be. A client might learn to respond to an event—for example, a relationship failure—in the same way that they might to a catastrophic event, even though a failed relationship had never previously entailed a horrible outcome. Its implications for therapy are just beginning to emerge (Hayes et al. 1999). The promise of the exploration of the relational operant in the analysis of language and therapy is one of the more interesting innovations for those doing research on the cutting edge of operant theory.
In the last decade, an analysis of how to apply operant learning principles in interpersonal psychotherapy has also begun. Kohlenberg and Tsai (1991) have detailed functional analytic psychotherapy, which describes the reinforcing functions of the therapeutic relationship that the therapist can use to affect significant behavior change in adult outpatient populations.
Advances in basic operant research are emerging at an increasing rate. Innovations in therapy are addressing new classes of problems that have not previously been the focus of an operant analysis. The role of operant conditioning will continue to maintain a prominent position in applied clinical psychology.
Bibliography:
- Allyon T, Azrin N H 1968 The Token Economy: A Motivational System for Therapy and Rehabilitation. Appleton-CenturyCrofts, New York
- Barlow D H 1990 Anxiety and its Disorders: The Nature and Treatment of Anxiety and Panic. Guilford, New York
- Barnes-Holmes D, Hayes S C, Hegarty N, Dymond S (in press) Multiple stimulus relations, the transformation of stimulus functions, and the limits of class concept. In: Hayes S C, Barnes-Holmes D (eds.) Relational Frame Theory: Creating a New Behavioral Agenda in Language and Cognition. Context, Reno, NV
- Ferster C B, Skinner B F 1957 Schedules of Reinforcement. Appleton-Century-Crofts, New York
- Foa E B, Steketee G, Milby J B 1980 Differential effects of exposure and response prevention in obsessive-compulsive washers. Journal of Consulting and Clinical Psychology 48: 71–9
- Hayes S C, Brownstein A J 1986 Mentalism, behavior-behavior relations and a behavior analytic view of the purposes of science. The Behavior Therapist 9: 175–90
- Hayes S C, Strosahl K D, Wilson K D 1999 Acceptance and Commitment Therapy: An Experiential Approach to Behavior Change. Guilford, New York
- Kanfer F H, Saslow G 1969 Behavioral diagnosis. In: Franks C M (ed.) Behavior Therapy: Appraisal and Status. McGrawHill, New York, pp. 417–44
- Kohlenberg R J, Tsai M 1991 Functional Analytic Psycho-therapy. Plenum, New York
- Lovaas O I 1977 The Autistic Child: Language Development Through Behavior Modification. Irvington, New York
- Lovaas O I 1987 Behavioral treatment and normal educational and intellectual functioning in young autistic child. Journal of Consulting and Clinical Psychology 55: 3–9
- Miller W R, Zweben A, DiClemente C C, Rychtarik R G 1992 Motivational Enhancement Therapy Manual. A Clinical Research Guide for Therapists Treating Individuals with Alcohol Abuse and Dependence. National Institute of Alcohol Abuse and Alcoholism, Rockville, MD, Vol. 2
- Sidman M 1986 Functional analysis of emergent verbal classes. In: Thompson T, Zeiler M D (eds.) Analysis and Integration of Behavioral Units. Erlbaum, Hillsdale, NJ, pp. 213–45
- Sidman M 1994 Stimulus Equivalence: A Research Story. Authors Cooperative, Boston
- Skinner B F 1945 The operational analysis of psychological terms. Psychological Review 52: 270–7
ORDER HIGH QUALITY CUSTOM PAPER

Always on-time

Plagiarism-Free

100% Confidentiality